
Endometrioid adenocarcinoma with sacral metastasis
Endometroidní adenokarcinom s metastázou v křížovém obratli
Většina nádorů kostí jsou metastázy. Primární nádory, které tvoří metastázy v kostech, se nejčastěji vyskytují v prsu, plicích, ledvinách a štítné žláze. Tato případová studie popisuje pacientku s výskytem nádoru kosti v osové kostře, původně v křížové oblasti. Primární místo nebylo určeno. Vyšetření tedy bylo nutné rozšířit o imunohistochemii, která prokázala metastatický nádor kompatibilní s endometroidním adenokarcinomem, nicméně ani po vyšetřeních nebyla v oblasti endometria nalezena aktivní léze. Tato studie byla observační a popisná, s cílem rozebrat důležitost přesnějších vyšetřovacích metod. V tomto směru imunohistochemie vyniká jako precizní metoda schopná optimalizovat diagnózu, léčbu a následně i prognózu.
Klíčová slova:
imunohistochemie – novotvar kostí – endometrioidní adenokarcinom
Authors:
Lorayne Cardoso Gontijo 1
![]() ; Renata Margarida Etchebehere 2
; Renata Margarida Etchebehere 2
![]() ; Luís Ronan Marquez Ferreira de Souza 3
; Luís Ronan Marquez Ferreira de Souza 3
![]() ; Eddie Fernando Candido Murta 1
; Eddie Fernando Candido Murta 1
![]() ; Rosekeila Simões Nomelini 1,4
; Rosekeila Simões Nomelini 1,4
![]()
Authors‘ workplace:
Laboratory of Applied Sciences for Women (LaCam)/ Department of Gynecology and Obstetrics, Federal University of Triângulo Mineiro, Uberaba-MG, Brazil
1; Surgical Pathology Service, Federal University of Triângulo Mineiro, Uberaba-MG, Brazil
2; Discipline of Radiology, Federal University of Triângulo Mineiro, Uberaba-MG, Brazil
3; Graduate Program in Gynecology and Obstetrics of the Ribeirão Preto Medical School of the University of São Paulo (FMRP-USP), Ribeirão Preto, São Paulo, Brazil
4
Published in:
Ceska Gynekol 2024; 89(4): 298-303
Category:
Case Report
doi:
https://doi.org/10.48095/cccg2024298
Overview
Most bone tumors are metastatic. Breasts, lungs, kidneys, and thyroid are the primary sites most commonly involved in bone metastasis-type outcomes. This case study describes the involvement of a patient with a bone tumor located in the axial skeleton, initially in the sacral region. However, the primary site was undefined. Therefore, it was necessary to expand the investigation with immunohistochemistry, which demonstrated a metastatic tumor compatible with endometrioid adenocarcinoma. But even after examination, no active lesion was found in the endometrial region. The study was observational, descriptive, and aimed to discuss the importance of more specific investigative methods. In this context, immunohistochemistry stands out as an exquisite method capable of optimizing diagnosis, therapy, and consequently, prognosis.
Keywords:
immunohistochemistry – bone neoplasm – endometrioid adenocarcinoma
Introduction
Metastatic tumor dissemination involves steps that include oncogenesis, angiogenesis, growth speed, presence of tumor cells with properties of both invasion and adhesion to the target tissue, and interaction with the host‘s immune system [1]. Patients who are unaware that they have any neoplasms may develop symptoms restricted to metastatic disease. Initial symptoms may include severe and disabling pain, resulting from nerve compression by the tumor mass, in addition to hypercalcemia and pathological fractures [2].
Metastatic bone tumor is most likely to originate from the breast, lung, prostate, kidney, or thyroid. However, other types of gynecological cancers can also spread to bone regions, mainly through hematogenous dissemination. When patients with endometrial cancer present with tumor metastases, involvement of the lungs, liver, central nervous system, and bones is most commonly expected [3]. Bone metastases are generally restricted to the axial skeleton, including the skull, ribs, spine, pelvis, humerus, and femur. Occurrence of bone metastases from endometrial adenocarcinoma emphasizes that sacral involvement is very rare [4].
Therefore, this present report aims to describe the case of a patient affected by neoplastic bone infiltration initially located in the sacral region, which was investigated based on the trigger of severe pain in the lower limb. The primary site of the lesion was unknown. Therefore, it was necessary to use immunohistochemistry to assist in diagnosis, conduct therapy, and consequently, assist in defining the prognosis.


Own observation
A 56-year-old woman G2P2, was seen at the UFTM Gynecological Oncology outpatient clinic, referred from the department of Orthopedics. The patient complained of disabling pain in the sacral region radiating to the right lower limb, resulting in bed confinement. The patient had menopause in 2016, and did not use hormone replacement therapy. She had minor intermittent transvaginal bleeding in 2018, and a transvaginal ultrasound was performed showing endometrial thickening (10.4 mm). She underwent endometrial biopsy at another location, and histopathology showed an endometrial polyp without atypia.
There were no new episodes of transvaginal bleeding, but she started having hip pain, which progressed to the entire right lower limb. She underwent magnetic resonance imaging of the lumbar spine in 2020, which found heterogeneous expansive lesions in the sacrum and iliac on the right. The diagnostic hypothesis was secondary implants. The biopsy of the sacral lesion suggested metastasis of an endometrioid adenocarcinoma with squamous differentiation, with the uterus as the probable primary site.
Transvaginal ultrasound showed normal thickness of the endometrium (3 mm) and preserved uterine volume. Pelvic MRI showed a sacral infiltrative neoplastic solid mass related to a secondary implant with lobulated contours, determining destruction from S2 to S5 with invasion of the vertebral canal and an extensive area of central hemorrhagic necrosis measuring 14.1 × 10.8 cm. It had an extensive extra-osseous component, eroding the most posterior region of the iliac bones and entrapping neural roots from S2 to S4, as well as the sciatic nerves (Fig. 1, 2).
Upper digestive endoscopy and colonoscopy did not demonstrate neoplasia. Current and previous 2-year Pap smears were normal. Chest tomography was normal. Abdominal computed tomography showed a uterus with intramural leiomyomas, there was no free fluid or retroperitoneal lymph node enlargement, and multiple bone lesions in the pelvis were seen, suggestive of secondary implants. PET-CT showed glycolytic hypermetabolism in the periphery of a voluminous expansive formation in the pelvis, consistent with a process of neoplastic nature; there were hypermetabolic lytic lesions in the right iliacus, pubis, and ischium and in the medial malleolus of the left tibia consistent with secondary lesions. No uterine changes were detected.
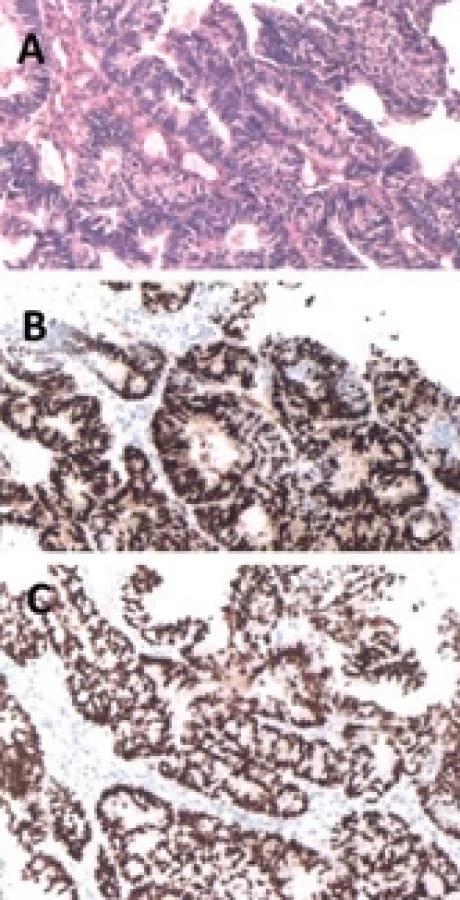
An endometrial biopsy slide review previously performed in 2019 was performed, which demonstrated an endometrial polyp with cystic dilation of glands and tubal metaplasia. Material from the sacral region submitted for analysis by immunohistochemistry revealed expression of PAX8 and estrogen receptor, which were findings compatible with metastatic adenocarcinoma, favoring origin in the female genital tract, especially the endometrium (Fig. 3).
After extensive discussion about initiating the best therapy, it was decided to submit the patient to radiotherapy (10 sessions), followed by chemotherapy (paclitaxel and carboplatin). After treatment, magnetic resonance imaging of the pelvis showed a reduction in metastatic lesions.
At the end of 2022, the patient began to experience pain in her left ankle. An X-ray was performed showing a destructive lytic lesion with large bone resorption in the region of the left distal tibia. A biopsy was performed, where the result was compatible with metastasis of endometrioid adenocarcinoma with squamous differentiation, and radiotherapy was initiated. In March 2023, the patient presented with exposure of a tumor in the distal tibia, requiring infragenicular amputation of the left lower limb. As a gynecological oncology approach, hormone therapy with megestrol acetate was started in April 2023, and a biphosphonate was started (pamidronate). The patient continues to be monitored jointly with orthopedics, gynecology, and oncology, and continues to undergo serial imaging tests, with no new tumor findings.
Discussion
According to data from the National Cancer Institute (NIH-USA), the estimated incidence of endometrial cancer is 3.4% in 2023. The average age of affected women is around 63 years. Regarding staging, 67% of cases are confined to the endometrium and only 10% of cases are considered distant metastases [5].
Transvaginal bleeding is generally the first symptom of patients affected by endometrial cancer and can occur due to endometrial thickening, resulting from disordered tissue proliferation, mediated by excess estrogen. Obesity is a risk factor for the development of endometrial cancer, as well as insulin resistance and high blood pressure [6].
In women with postmenopausal bleeding, transvaginal ultrasound is considered a highly sensitive test for diagnosing endometrial cancer. According to ACOG (American College of Obstetricians and Gynecologists), if transvaginal ultrasound in a patient with postmenopausal bleeding shows endometrial thickness of 4 mm or less, endometrial sampling is not necessary due to the very low risk of malignancy in these patients. On the other hand, if the endometrial thickness is greater than 4 mm, an endometrial evaluation should be performed, such as hysteroscopy and endometrial biopsy. However, the significance of endometrial thickness greater than 4 mm in an asymptomatic postmenopausal patient has not been established [7].
Approximately 60% of uterine curettage samples are not able to reveal more than half of the uterine cavity. Thus, hysteroscopy-directed biopsy is a more sensitive method than curettage for diagnosing uterine lesions [8]. Sensitive and accurate diagnosis of true premalignant endometrial lesions can reduce the likelihood of developing invasive endometrial cancer. Based on available data and expert opinion, the American College of Obstetricians and Gynecologists and the Society of Gynecologic Oncology make the following consensus recommendations: give preference to hysteroscopy, in order to include any discrete lesions and avoid false negative results. When clinically appropriate, total hysterectomy for endometrial intraepithelial neoplasia provides definitive evaluation of possible concomitant carcinoma and effectively treats premalignant lesions [9].
The patient in our report presented with postmenopausal bleeding and ultrasound showed significant endometrial thickening. However, the cavity investigation was performed only with uterine curettage and without hysteroscopy. One hypothesis is that there was a false negative in this test, and malignant cells may have reached the blood vessels and metastasized, and subsequently the disease regressed locally due to the anti-tumor immune response itself.
After defining the diagnosis, it is essential to stage the disease, as this defines the choice of treatment. The long-term survival of endometrial cancer patients is strongly related to the stage of the disease at the time of diagnosis. Endometrial cancer staging is performed surgically and includes peritoneal fluid cytology, biopsy of suspicious lesions (intra - or retroperitoneal), total extrafascial hysterectomy, bilateral adnexectomy, and pelvic and para-aortic lymphadenectomy [10].
Distant endometrial cancer metastases most commonly involve the lung, liver, bone, and brain. However, bone metastases occur in less than 15% of patients [3]. The types of cancer that most often cause bone metastases are breast, prostate, lung, thyroid, and kidney, a fact that can be explained by the affinity of cancer cells from these origins for bone tissue cells. In this context, the bone scintigraphy test is highly sensitive in detecting bone metastases, despite being not very specific [1].
In our case study, the diagnosis began with the finding of metastases, and consequently, triggered an extensive propaedeutic investigation, in order to clarify the initial topography of the tumor. Special attention was given to the uterine cavity due to previous history; however, no lesion other than bone was found. It is estimated that approximately 4% of all patients with neoplasms have carcinomas of unknown origin. Identification of the primary site is of great clinical relevance, as it directly affects prognosis and treatment [11].
Integrating morphology with immunohistochemistry, the pathologist is generally able to provide definitive diag - nostic information about the most likely primary site of the carcinoma that presented as metastases. Therefore, immunohistochemistry is considered the gold standard in the diagnosis of cancers of unknown primary site [11]. Immunohistochemistry is necessary when diagnosis is difficult in unknown primary cancers or in cases with multiple cancers. It is based on the identification of predictive and prognostic biomarkers from tumor samples to define treatment and establish the prognosis of the disease [12]. The immunohistochemistry report in this case demonstrated histological aspects compatible with adenocarcinoma metastasis, favoring a primary site in the endometrium with positivity in the PAX8 and estrogen receptor markers.
Tumors originating in the female genital tract generally exhibit nuclear expression for estrogen receptors (ER). Immunohistochemistry is utilized to define primary tumor sites, saying that endometrial carcinomas of the endometrioid type (type 1) present reactivity to estrogen receptors, while serous and clear cell uterine carcinomas (type 2) generally do not express such receptors [13]. The evaluation of the estrogen receptor using the immunohistochemistry method can be part of a panel, which also includes monoclonal carcinoembryonic antigen, vimentin, and p16, to differentiate endometrial adenocarcinoma from endocervical adenocarcinoma. This is because endometrioid carcinomas are usually diffusely ER positive, while endocervical adenocarcinomas are ER negative [14]. PAX8 is a transcription factor involved in the organogenesis of the thyroid/parathyroid, kidneys, and female genital tract (Mullerian system). After genital formation, it remains expressed in non-ciliated mucous cells of the fallopian tubes, endocervix, endometrium, and ovaries [15]. Regarding PAX8 expression in gynecological cancers, Kandalaft et al. (2016) stated that it was positive mainly in non-mucinous ovarian cancers, endometrial, and clear cell adenocarcinoma [13].
Regarding the treatment of endometrial tumors, surgery defines the staging and in many cases it is the gold standard for treatment. According to Shah (2011), performing total hysterectomy plus bilateral salpingo-oophorectomy, associated with lymphadenectomy, is a traditional treatment for operable tumors. However, in patients with distant metastases (FIGO stage IV), as in the case of the patient in the aforementioned report, the therapeutic option does not include surgical resection of the uterus and adnexa [16]. According to the Society of Gynecologic Oncology Clinical Practice Committee (SGO), inoperable gynecological tumors can be treated with systemic chemotherapy. However, the choice of therapeutic regimen is controversial since these patients form a heterogeneous group and metastases can be distributed to different locations among those with advanced-stage neoplasia. This causes difficulty in standardizing management. The SGO discusses the use of chemotherapy in patients with metastatic endometrial cancer and explains that among the chemotherapy drugs available for this purpose, the combination of paclitaxel and carboplatin presents a good response associated with less toxicity when compared to other regimens [17].
Radiotherapy is also part of the therapeutic arsenal. It can be used concomitantly with chemotherapy. In the case of the patient in question, pelvic radiotherapy was not indicated due to the absence of evidence of an active endometrial lesion. However, radiotherapy treatment was indicated for metastatic lesions in bone tissue, together with chemotherapy (paclitaxel and carboplatin). Radiotherapy, used for metastatic bone tumors, according to Shibata et al. (2016) can promote tumor reduction, pain control, and prevention of secondary pathological fractures [2]. There are different therapeutic methods that aim to control the pain of bone metastasis and contain bone destruction, such as opioid analgesics, chemoradiotherapy, and hormonal therapy [18].
Megestrol acetate is a synthetic progestin that has an antagonistic action against estrogen in the endometrium. It can be used for adjuvant treatment of endometrial cancer. However, most studies restrict such therapy to less invasive tumors and patients without defined offspring. The use of megestrol acetate, associated with hysteroscopic resection, is effective in conservative treatment of tumors in the early and pre-malignant stages [19]. Shah (2011) compares studies that analyze different progestins (megestrol acetate, medroxyprogesterone, and intrauterine levonogestrel) and highlights such therapeutic possibilities for patients with a desire for ovarian preservation or those with inoperable tumors [16].
In our patient, the persistence of the progression of bone disease to the tibial region was a fundamental fact in the decision to add another bone therapy. Regarding bone modifying drugs, the American Society of Clinical Oncology (ASCO) recommends the use of Denosumab 120 mg subcutaneously every four weeks, Zolendronic Acid 4 mg every four weeks or every 12 weeks, or intravenous Pamidronate 90 mg every four weeks. Pamidronate disodium is a second generation bisphosphonate with the ability to control and cause apoptosis of osteoclasts. Currently, the bisphosphonates mostly used in clinical practice include Pamidronate disodium, Ibandronate sodium, Zoledronic Acid, and Incardronate disodium [18]. The treatment of metastatic bone lesions, in the absolute majority, does not lead to a cure due to the already advanced stage of the tumor disease. Surgery may be necessary for tumor excision or bone fixation [20]. However, despite the severity of the cases, early treatment is imperative, as it aims to control pain, preserve function, and maintain quality of life.
The prognostic factors of patients with endometrial cancer associated with bone metastases highlight the importance of considering such a diagnosis in the face of recurrent complaints of musculoskeletal pain, especially in postmenopausal women. Accurate diagnosis and early treatment can result in a better prognosis [21].
Conclusion
This case study elucidates some fundamental points regarding the approach to studying endometrial cancer: diag-nostic methods, staging, work-up methods, treatment, and prognosis. In the case in question, there was a finding of endometrial hyperplasia associated with the presence of a polyp. The patient had no major risk factors for developing endometrial cancer, just age and hypertension. Furthermore, the case in question offers us an intriguing and unexpected result due to the absence of an active uterine lesion and metastatic tumor with a primary focus on the endometrial site, requiring confirmation by immunohistochemistry. Bone metastases, mainly sacral and of endometrial focus are rare, especially in the context presented without evidence of an active endometrial lesion. There are no reports of similar cases available in the databases prior to the present report. Due to the rarity of the case under analysis, it is difficult to conclude on the prognostic factors or effective treatments that will impact the survival and quality of life of the patient.
Sources
1. Macedo F, Ladeira K, Pinho F et al. Bone metastases: an overview. Oncol Rev 2017; 11 (1): 321. doi: 10.4081/oncol.2017.321.
2. Shibata H, Kato S, Sekine I et al. Diagnosis and treatment of bone metastasis: comprehensive guideline of the Japanese Society of Medical Oncology, Japanese Orthopedic Association, Japanese Urological Association, and Japanese Society for Radiation Oncology. ESMO Open 2016; 1 (2): e000037. doi: 10.1136/esmo open-2016-000037.
3. Hacker NF. Uterine cancer. In: Berek JS, Hacker NF (eds). Practical gynecologic oncology. Philadelphia, PA: Lippincott Williams & Wilkins 2005 : 397–442.
4. Albareda J, Herrera M, Lopez Salva A et al. Sacral metastasis in a patient with endometrial cancer: case report and review of the literature. Gynecol Oncol 2008; 111 (3): 583–588. doi: 10.1016/j.ygyno.2008.04.005.
5. NIH-USA National Cancer Institute, Surveillance, Epidemiology, and End Results Program, Cancer Stat Facts: Uterine Cancer. 2023 [online]. Available from: https: //seer.cancer.gov/statfacts/html/corp.html.
6. Sorosky JI. Endometrial cancer. Obstet Gynecol 2012; 120 (2 Part 1): 383–397. doi: 10.1097/ aog.0b013e3182605bf1.
7. ACOG (American College of Obstetricians and Gynecologists). Committee on Gynecologic Practice. Society of Gynecologic Oncology. 2020 [online]. Available from: https: //www.acog.org/clinical/clinical-guidance/committee-opinion.
8. Bedner R, Rzepka-Górska I. Hysteroscopy with directed biopsy versus dilatation and curettage for the diagnosis of endometrial hyperplasia and cancer in perimenopausal women. Eur J Gynaecol Oncol 2007; 28 (5): 400–402.
9. ACOG (American College of Obstetricians and Gynecologists). The role of transvaginal ultrasonography in the evaluation of postmenopausal bleeding. ACOG Committee Opinion No. 440. 2018 [online]. Available from: https: //www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2018/05/the-role-of-transvaginal-ultrasonography-in-evaluating-the-endometrium-of-women-with-postmenopausal-bleeding.
10. Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet 2009; 105 (2): 103–104. doi: 10.1016/j.ijgo.2009.02.012.
11. Weiss LM, Chu P, Schroeder BE et al. Blinded comparator study of immunohistochemical analysis versus 92-gene cancer classifier in the diagnosis of the primary site in metastatic tumors. J Mol Diagn 2013; 15 (2): 263–269. doi: 10.1016/j.jmoldx.2012.10.001.
12. Werner M, Chott A, Fabiano A et al. Effect of formalin tissue fixation and processing on immunohistochemistry. Am J Surg Pathol 2000; 24 (7): 1016–1019. doi: 10.1097/00000 478-200007000-00014.
13. Kandalaft PL, Gown AM. Practical applications in immunohistochemistry: carcinomas of unknown primary site. Arch Pathol Lab Med 2016; 140 (6): 508–523. doi: 10.5858/arpa. 2015-0173-CP.
14. McCluggage WG, Palaniappan Sumathi V, McBride HA et al. Panel of immunohistochemical stains, including carcinoembryonic antigen, vimentin, and estrogen receptor, aids the distinction between primary endometrial and endocervical adenocarcinomas. Int J Gynecol Pathol 2002; 21 (1): 11–15. doi: 10.1097/00004347-200201000-00003.
15. Ordóñez NG.Value of PAX 8 immunostaining in tumor diagnosis: a review and update. Adv Anat Pathol 2012; 19 (3): 140–151. doi: 10.1097/ PAP.0b013e318253465d.
16. Shah MM, Wright JD. Management of endometrial cancer in young women. Clin Obstet Gynecol 2011; 54 (2): 219–225. doi: 10.1097/GRF.0b013e318218607c.
17. SGO Clinical Practice Endometrial Cancer Working Group, Burke WM, Orr J, Leitao M et al. Endometrial cancer: a review and current management strategies: part II. Gynecol Oncol 2014; 134 (2): 393–402. doi: 10.1016/ j.ygyno.2014.06.003.
18. Wang Y, Tang Z, Meng R et al. Side effects of incardronate disodium compared to pamidronate disodium in the treatment of bone metastasis pain: a systematic review and meta-analysis. Ann Palliat Med 2021; 10 (11): 11950–11959. doi: 10.21037/apm-21-3056.
19. Masciullo V, Trivellizzi N, Zannoni G et al. Prognostic impact of hysteroscopic resection of endometrial atypical hyperplasia-endometrioid intraepithelial neoplasia and early-stage cancer in combination with megestrol acetate acetate. Am J Obstet Gynecol 2021; 224 (4): 408–410. doi: 10.1016/j.ajog. 2020.12.1210.
20. Healey JH, Brown HK. Complications of bone metastases: surgical management. Cancer 2000; 88 (12 Suppl): 2940–2951. doi: 10.1002/1097-0142 (20000615) 88 : 12+<29 40:: aid-cncr10> 3.0.co; 2-w.
21. Basarir OZ, Karaca MO, Balaban K et al. Prognostic factors in endometrial cancer patients with bone metastasis. Jt Dis Relat Surg 2023; 34 (1): 207–214. doi: 10.52312/jdrs.2023.792.
Labels
Paediatric gynaecology Gynaecology and obstetrics Reproduction medicineArticle was published in
Czech Gynaecology

2024 Issue 4
Most read in this issue
- Movements of the pelvic bones of expectant mothers during vaginal delivery
- Preoperative discrimination between uterine myomas and sarcomas
- Incidence of stress urinary incontinence after laparoscopic sacrocolpopexy
- Surgical treatment of recurrent gynecological malignancies