
Atypical eclampsia without severe hypertension – the role of ophthalmic artery Doppler and sFlt-1/PlGF ratio: a case report
Authors:
V. Oom 1
![]() ; C. Fernandes 1
; C. Fernandes 1
![]() ; E. Araujo Júnior 2,3; Gustavo Yano Callado 4
; E. Araujo Júnior 2,3; Gustavo Yano Callado 4
![]() ; S. Proença 1
; S. Proença 1
![]() ; C. Nascimento 1
; C. Nascimento 1
![]() ; R. A. M. De Sá 5
; R. A. M. De Sá 5
![]() ; F. Nunes 1
; F. Nunes 1
![]()
Authors‘ workplace:
Service of Gynecology and Obstetrics, Cascais Hospital Dr. José de Almeida, Cascais, Portugal
1; Department of Obstetrics, Paulista School of Medicine – Federal University of São Paulo (EPM-UNIFESP), São Paulo-SP, Brazil
2; Discipline of Woman Health, Municipal University of São Caetano do Sul (USCS), São Caetano do Sul-SP, Brazil
3; Albert Einstein Israelite College of Health Sciences (FICSAE), Albert Einstein Israelite Hospital, São Paulo-SP, Brazil
4; Department of Clinical Research, National Institute of Women's, Children's and Adolescents' Health Fernandes Figueira, Oswaldo Cruz Foundation (IFF/Fiocruz), Rio de Janeiro-RJ, Brazil
5
Published in:
Ceska Gynekol 2026; 91(3): 181-185
Category:
Original Article
doi:
https://doi.org/10.48095/cccg2026181
Overview
Eclampsia remains one of the most severe obstetric emergencies associated with substantial maternal and perinatal morbidity and mortality. Although classically regarded as a hypertensive complication of pre-eclampsia, atypical presentations without sustained hypertension or severe clinical features may occur, complicating risk prediction and timely intervention. We report a case of atypical eclampsia in a 21-year-old woman hospitalized with a diagnosis of pre-eclampsia without severe features. Despite predominantly normal blood pressure values and initially stable laboratory findings, the sFlt-1/PlGF ratio and Doppler assessment of the uterine and ophthalmic arteries revealed significant abnormalities. The patient subsequently developed generalized tonic–clonic seizures, requiring urgent obstetric intervention. This case underscores the limitations of conventional diagnostic criteria in identifying patients at risk for sudden neurological deterioration and highlights the potential value of angiogenic biomarkers and targeted Doppler evaluation in refining risk stratification among women with pre-eclampsia.
Keywords:
Eclampsia – atypical presentation – sFlt-1/PlGF ratio – uterine artery Doppler – ophthalmic artery Doppler
Introduction
Pre-eclampsia and eclampsia are classically understood as hypertensive disorders of pregnancy that occur along a continuum of severity, with seizures representing the extreme manifestation of disease progression [1,2]. However, growing evidence indicates that this paradigm does not fully capture the clinical heterogeneity of these conditions. A substantial proportion of women who develop eclampsia do not present with antecedent hypertension or proteinuria, and seizures may occur abruptly, without prodromal symptoms or laboratory evidence of severe disease [3–6].
This diagnostic ambiguity poses a significant challenge in clinical practice, particularly when pregnant women develop end-organ dysfunction in the absence of sustained hypertension. Although clinical assessment and routine laboratory evaluation remain the cornerstone of risk stratification worldwide [7], emerging biomarkers and imaging modalities may provide additional insight into disease severity. Among these, the angiogenic imbalance reflected by the soluble fms-like tyrosine kinase-1/placental growth factor (sFlt-1/PlGF) ratio and Doppler assessment of maternal cerebrovascular circulation have gained increasing attention [8,9].
We report a case of atypical eclampsia in a normotensive patient initially diagnosed with pre-eclampsia without severe features, highlighting the limitations of conventional diagnostic criteria and the potential role of adjunctive tools in anticipating sudden neurological deterioration.
Case report
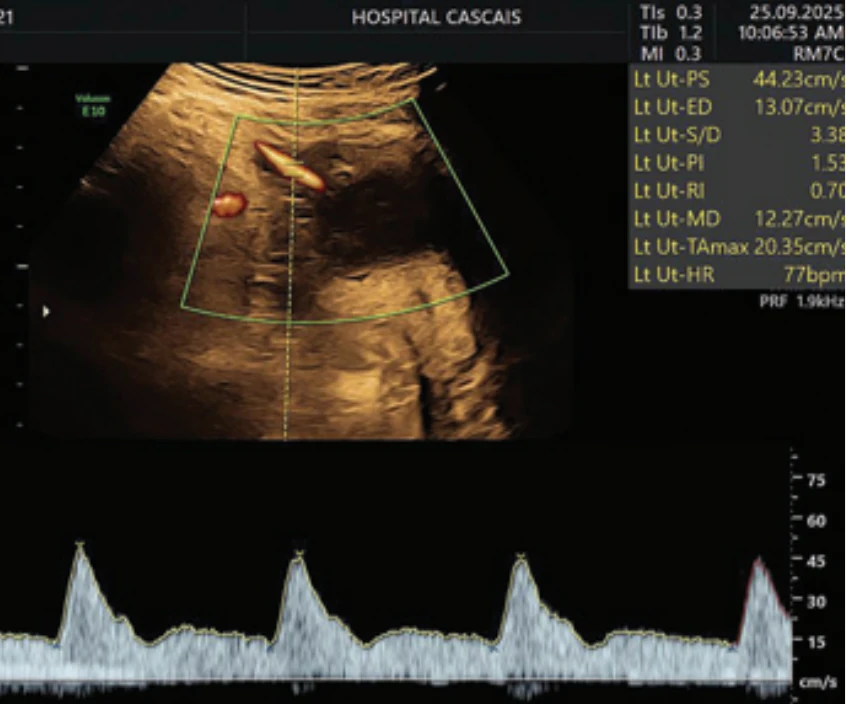
A 21-year-old gravida 1, para 0 from India was referred to our hospital for investigation due to early fetal growth restriction (estimated fetal weight by ultrasound at the 0.3rd percentile and umbilical artery pulsatility index above the 95th percentile) at 30 weeks and 5 days of gestational age, estimated by 1st trimester ultrasound. The patient also presented a mean pulsatility index of the uterine arteries above the 95th percentile at Doppler evaluation and amniotic fluid volume was normal (Fig. 1). It was initially a twin pregnancy up to 8 weeks. The clinical examination at the time of admission showed normal blood pressure values without medication and a closed cervix, without detectable bleeding. Cardiotocography showed a reactive pattern with no uterine activity. She was admitted with an initial diagnosis of preeclampsia without severe symptoms and a pulmonary maturation cycle with corticosteroids was done.
An emergency blood work was carried out, with the result of hemoglobin at 12.4 g/dL, 197,000 platelets/mm3, aspartate aminotransferase (AST) at 25 UI/L, alanine aminotransferase (ALT) 23 UI/L, lactate dehydrogenase (LDH) at 194 U/L, 0.5 mg/L of creatinine, a total bilirubin of 0.20 mg/dL, sFlt/PlGF ratio at 507 and a 24 h urinary protein of 1,622 mg/24 h.
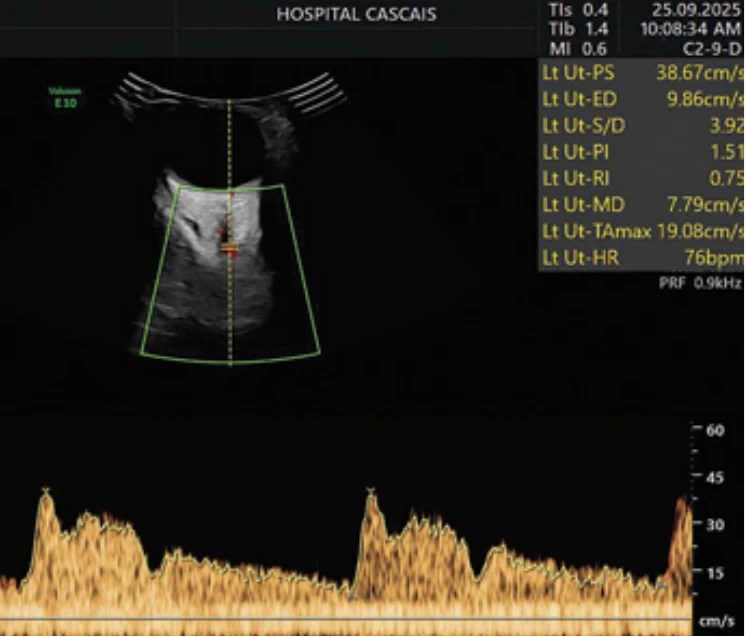
During the next 6 days she continued to be monitored through laboratory tests that showed similar results than those on admission, with exception for an elevation in uric acid (6.3 mg/dL) on the fourth day of hospitalization and a decrease in platelet count to 137,000, associated with an increase in the sFlt1/PlGF ratio to 706. Her blood pressure remained mostly normal throughout this period except for three episodes of an isolated registration of systolic blood pressure peaked (maximum 148 mmHg) and one evening with 154/105 mmHg, not confirmed in the next measurement, so no antihypertensive drug therapy was initiated. Although not part of the evaluation protocol, ophthalmic artery (OA) Doppler was performed on the fourth day of hospitalization in both eyes and we calculated the mean from Doppler indices: the mean PR index was 0.77, and the mean PSV2 was 25 cm/s (Fig. 2). These findings raised strong suspicion of progression to severe preeclampsia, despite the absence of hypertension or signs of severe pre-eclampsia in blood analyses.
The patient developed seizures on the seventh day of hospitalization and was diagnosed with eclampsia, requiring magnesium sulfate treatment after an acute episode of tonic-clonic seizure. The patient then underwent an emergent cesarean delivery at 31 weeks and 5 days. On postoperative day 1, the patient’s transaminases peaked with AST 37 U/L and ALT 26U/L; her LDH increased to 273 U/L. On postoperative day 2, the patient’s transaminases began to trend downwards and her mental status improved. At the time of discharge on postoperative day 6, her AST was 22 U/L, ALT was 31 U/L and LDH was 295 U/L. On postoperative day 4 her diastolic blood pressure was 94 mmHg and nifedipine 30 mg once a day was started. Her blood pressures remained normal during the rest of her hospital stay.
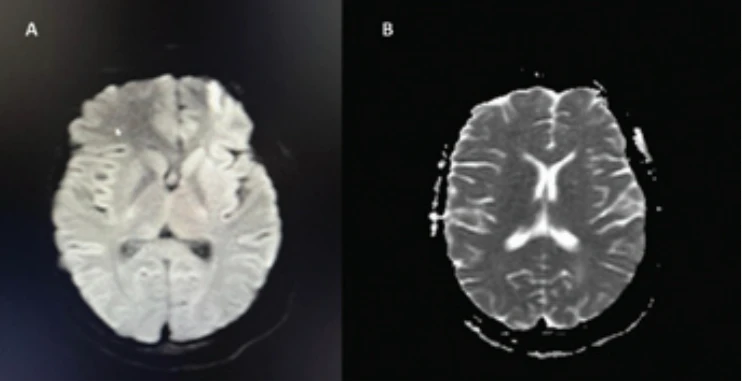
Magnetic resonance imaging (MRI) revealed focal ischemic brain lesions, including a corticospinal frontal right encephaloclastic lesion, suggesting possible vascular sequelae, as well as an older ischemic lesion in the left posterior periventricular region (Fig. 3).
Histopathological examination of the placenta showed a preterm simple placenta with a weight between the 10–25th percentiles for gestational age. Microscopic evaluation demonstrated accelerated villous maturation with placental infarcts, findings indicative of poor utero-placental perfusion.
After discharge, the patient’s blood analyses were found normal, and no further seizures occurred.
Discussion
This case illustrates a critical limitation of the traditional conceptualization of pre-eclampsia and eclampsia as disorders defined primarily by hypertension and overt laboratory abnormalities. Although pre-eclampsia has historically been framed as a progressive hypertensive condition culminating in seizures, contemporary data challenge this linear model. Between 20% and 38% of women who experience eclamptic seizures lack prior hypertension or proteinuria, and only a small fraction of patients with pre-eclampsia progress to eclampsia in randomized clinical trials [4–6,10–12]. Moreover, up to 40% of eclamptic events occur without warning symptoms such as headache, visual disturbances, or epigastric pain [3–6]. The present case exemplifies this atypical trajectory, with abrupt onset of seizures despite predominantly normal blood pressure values and initially stable laboratory parameters.
The diagnostic complexity of such presentations is further compounded by the overlap between hypertensive disorders of pregnancy and other obstetric or systemic conditions, including thrombotic thrombocytopenic purpura, hemolytic uremic syndrome, acute fatty liver of pregnancy, and autoimmune disease [1–3]. In this context, reliance solely on blood pressure thresholds and conventional laboratory markers may delay recognition of impending neurological complications. This challenge is particularly relevant given the persistent maternal and perinatal morbidity associated with eclampsia, even in high-resource settings [1,3,13].
Angiogenic imbalance has emerged as a key pathophysiological mechanism underlying placental dysfunction in pre-eclampsia. Elevated sFlt-1 levels and reduced PlGF reflect impaired placentation and endothelial dysfunction, correlating with disease severity and adverse outcomes [14]. In the present case, the markedly elevated sFlt-1/PlGF ratio, which continued to rise during hospitalization, suggested significant placental pathology despite the absence of sustained hypertension. These findings align with evidence supporting the role of angiogenic biomarkers as adjuncts for risk stratification, particularly in diagnostically ambiguous cases [7].
Beyond placental biomarkers, maternal cerebrovascular involvement is increasingly recognized as central to the pathogenesis of eclampsia. Eclamptic seizures are thought to result from blood-brain barrier dysfunction, impaired cerebral autoregulation, and increased vascular permeability, rather than from hypertension alone [3]. Ophthalmic artery Doppler ultrasound provides a noninvasive window into maternal cerebral hemodynamics, as the OA shares embryological and physiological characteristics with intracranial vessels [15,16]. Reduced resistance and increased diastolic flow in the OA have been interpreted as markers of cerebral vasodilation and hyperperfusion in pre-eclampsia [8,9].
In this patient, OA Doppler demonstrated a low pulsatility index and elevated PSV2, findings previously associated with adverse maternal outcomes. Naves et al. showed that OA Doppler parameters, particularly PSV2, can identify women at increased risk of clinical deterioration, even when conventional markers are inconclusive [8,9]. Importantly, these Doppler abnormalities preceded the onset of seizures in our case, suggesting that cerebrovascular changes may develop before overt neurological manifestations. While OA Doppler has not been shown to independently predict neonatal outcomes, its value in anticipating maternal complications appears clinically relevant [8,9].
Concomitantly, the elevated uterine artery pulsatility index observed in this patient reflected impaired uteroplacental perfusion, corroborated by histopathological findings of accelerated villous maturation and placental infarction. Uterine artery Doppler abnormalities are well-established markers of placental insufficiency and pre-eclampsia risk, reinforcing the concept that placental and maternal vascular dysfunction may evolve in parallel, yet manifest clinically at different times [1,7].
Taken together, this case supports a more integrated model of pre-eclampsia and eclampsia, in which angiogenic imbalance, placental dysfunction, and maternal cerebrovascular dysregulation may precede or occur independently of sustained hypertension. Incorporating adjunctive tools such as the sFlt-1/PlGF ratio, uterine artery Doppler, and ophthalmic artery Doppler into selected clinical scenarios may enhance early risk identification and allow for more individualized surveillance strategies. While these modalities should not replace clinical judgment or established diagnostic criteria, they may provide critical complementary information in atypical or equivocal cases.
Conclusion
This case underscores the need for an expanded diagnostic framework for pre-eclampsia and eclampsia that extends beyond blood pressure values and routine laboratory findings. In patients with atypical presentations, angiogenic biomarkers and Doppler assessment of uteroplacental and cerebrovascular circulation may offer valuable insights into disease severity and imminent risk. Integrating these tools into clinical practice, particularly for women with early placental dysfunction or unexplained clinical deterioration, may facilitate earlier intervention and contribute to improved maternal and perinatal outcomes.
Sources
1. Póvoa AM, Costa F, Rodrigues T et al. Prevalence of hypertension during pregnancy in Portugal. Hypertens Pregnancy 2008; 27 (3): 279–284. doi: 10.1080/10641950802000943.
2. Gestational hypertension and preeclampsia: ACOG practice bulletin, number 222. Obstet Gynecol 2020; 135 (6): e237–e260. Doi: 10.1097/AOG.00000000000038912.
3. Fishel Bartal M, Sibai BM. Eclampsia in the 21st century. Am J Obstet Gynecol 2022; 226 (2S): S1237–S1253. doi: 10.1016/j.ajog.2020.09.037.
4. Sibai BM, Stella CL. Diagnosis and management of atypical preeclampsia-eclampsia. Am J Obstet Gynecol 2009; 200 (5): 481.e1–481.e4817. doi: 10.1016/j.ajog.2008.07.0483.
5. Stella CL, Sibai BM. Preeclampsia: diagnosis and management of the atypical presentation. J Matern Fetal Neonatal Med 2006; 19 (7): 381–386. doi: 10.1080/147670506006783374.
6. Noraihan MN, Sharda P, Jammal AB. Report of 50 cases of eclampsia. J Obstet Gynaecol Res 2005; 31 (4): 302–309. doi: 10.1111/j.1447 - 0756.2005.00292.x5.
7. MacDonald TM, Walker SP, Hannan NJ et al. Clinical tools and biomarkers to predict preeclampsia. EBioMedicine 2022; 75 : 103780. doi: 10.1016/j.ebiom.2021.103780.
8. Monteiro VN, de Oliveira CA, Gomes Junior SC et al. Ophthalmic artery Doppler as a predictor of adverse neonatal outcomes in women with preeclampsia. J Clin Ultrasound 2025; 53 (3): 504–509. doi: 10.1002/jcu.23899.
9. Naves WU, Moreira RA, Monteiro VN et al. The use of Doppler velocimetry of the ophthalmic artery and the fullPIERS model to predict adverse outcomes in hospitalized pregnant women with preeclampsia: a prospective cohort study. J Matern Fetal Neonatal Med 2025; 38 (1): 2526112. doi: 10.1080/14767058.2025.2526112.
10. Sibai BM. Diagnosis, prevention, and management of eclampsia. Obstet Gynecol 2005; 105 (2): 402–410. doi: 10.1097/01.AOG.0000152351.13671.996.
11. Cooray SD, Edmonds SM, Tong S et al. Characterization of symptoms immediately preceding eclampsia. Obstet Gynecol 2011; 118 (5): 995–999. doi: 10.1097/AOG.0b013e31823245707.
12. Coetzee EJ, Dommisse J, Anthony J. A randomised controlled trial of intravenous magnesium sulphate versus placebo in the management of women with severe pre-eclampsia. Br J Obstet Gynaecol 1998; 105 (3): 300–303. doi: 10.1111/j.1471-0528.1998.tb10090.
13. Magee LA, Nicolaides KH, von Dadelszen P. Preeclampsia. N Engl J Med 2022; 386 (19): 1817–1832. doi: 10.1056/NEJMra2109523.
14. Binder J, Palmrich P, Kalafat E et al. Longitudinal assessment of angiogenic markers in prediction of adverse outcome in women with confirmed pre-eclampsia. Ultrasound Obstet Gynecol 2023; 62 (6): 843–851. doi: 10.1002/uog.26276.
15. Nicolaides KH, Sarno M, Wright A. Ophthalmic artery Doppler in the prediction of preeclampsia. Am J Obstet Gynecol 2022; 226 (2S): S1098–S1101. doi: 10.1016/j.ajog.2020.11.039.
16. Arkorful J, Browne JL, Adu-Bonsaffoh K et al. Predictive accuracy of ophthalmic artery Doppler for pre-eclampsia: a systematic review. BMJ Open 2025; 15 (6): e094348. doi: 10.1136/bmjopen-2024-094348.
Labels
Paediatric gynaecology Gynaecology and obstetrics Reproduction medicineArticle was published in
Czech Gynaecology
2026 Issue 3
Most read in this issue
- Syndrom amniálních pruhů – kazuistika prenatálně zjištěné amputace horní končetiny plodu
- Junctional zone thickness on magnetic resonance imaging – a non-invasive diagnostic method for adenomyosis and beyond
- Perinatální paliativní péče u pacientky s antenatálním úmrtím plodu v důsledku těžké preeklampsie s předčasným odloučením placenty
- Lichen sclerosus – pohľad dermatológa a terapeutické možnosti