
Results of the Endometriosis Health Profile-30 questionnaire in women aged 18– 30 years in the Czech Republic
Výsledky dotazníku „Endometrióza zdravotního profilu 30“ u žen ve věku 18 – 30 v České republice
Cíl: Cílem studie je získat validní data o kvalitě života žen ve věku 18–30 let s endometriózou pomocí certifikovaného dotazníku the Endometriosis Health Profile-30 (EHP-30). Ve studii byla použita česká verze dotazníku EHP-30. Dotazník vyplnilo 184 žen. Průměrný věk žen byl 26,6 let (± 2,8). Materiály a metody: Na českou verzi dotazníku EHP-30 jsme získali licenci od Oxfordské univerzity. Data byla sbírána od 10. února 2023 do 8. října 2023 pomocí online platformy Click4survey. Výsledky: Souhrnný index skupiny EHP-30 byl 57,0 bodů (± 20,43 bodu). Nejvíce kvalitu života žen ovlivňuje doména Bezmoci kontroly nad nemocí (66,4 bodů), dále Sociální podpora (58,4 bodů) a Emocionální pohoda (58,2 bodů). K závěrečným doménám patří Bolest (51,3 bodů) a Sebeobraz (50,7 bodů), který byl na posledním místě. Z výsledků vyplynulo, že vnímání bolesti se nezvyšuje s přibývajícím věkem, naopak nejhůře bolest vnímají ženy nejmladší věkové kategorie 18–20 let. Věk žen statisticky významně neovlivňoval výsledný index dotazníku ani jeho jednotlivé rozměry. Závěr: Na základě provedené analýzy a získaných výsledků jsme získali data o doménách endometriózy, což může významně přispět k efektivnějšímu porozumění možnosti zlepšení kvality života žen ve věku 18–30 let s endometriózou a postupů při jejich terapii.
Klíčová slova:
Endometrióza – bolest – sociální podpora – Endometriosis Health Profile-30 – kontrola a bezmoc
Authors:
Ingrid Palaščáková Špringrová 1,2
![]() ; Martin Němec 3
; Martin Němec 3
![]() ; Martina Kadlecová 4
; Martina Kadlecová 4
Authors place of work:
REHASPRING centrum s. r. o., Prague-East Čelákovice, Czech Republic
1; Department of Rehabilitation, Faculty of Health Studies, University of West Bohemia in Pilsen, Czech Republic
2; Department of Obstetric and Gynecology, Hospital Frýdek-Místek p. o., Czech Republic
3; Hospital Na Františku, Prague, Czech Republic
4
Published in the journal:
Ceska Gynekol 2025; 90(5): 380-384
Category:
Původní práce
doi:
https://doi.org/10.48095/cccg2025380
Summary
Aim: The aim of the study is to obtain valid data on the quality of life of women aged 18–30 years with endometriosis using the certified questionnaire the Endometriosis Health Profile-30 (EHP-30). The Czech version of the EHP-30 was used in the study. A total of 184 women completed the questionnaire. Mean age of the women was 26.6 years (± 2.8 years). Materials and methods: Data were collected from 10 February 2023 to 8 October 2023 using the online platform Click4survey. Results: Summary index of the EHP-30 group was 57.0 points (± 20.43 points). The domain of powerlessness to control the disease had the greatest impact on women‘s quality of life at 66.4 points, followed by Social support at 58.4 points, then Emotional well-being at 58.2 points. With Pain at 51.3 points, and Self-image at 50.7 points as the final domain. Results showed that perception of pain did not increase with increasing age, and on the contrary, women in the youngest age group of 18–20 years perceived pain as the worst. The age of women did not statistically significantly affect the final index of the questionnaire or its individual dimensions. Conclusion: Based on the analysis and results obtained, we have obtained data on the domains of endometriosis, which can significantly contribute to a more effective understanding of the possibility of improving the quality of life of women aged 18–30 years with endometriosis and the procedures for their treatment.
Keywords:
Endometriosis – Pain – social support – Endometriosis Health Profile-30 – control and powerlessness
Introduction
Endometriosis is a common disease that affects 5–10% of women of reproductive age worldwide. If we focus on the cohort of sterile women, we find endometriosis in up to 50% of cases. However, despite the prevalence, diagnosis is usually delayed by several years, misdiagnosis often occurs and the provision of effective treatment is prolonged. Endometriosis is a gynaecological disease caused by the implantation of active endometrial cells outside the uterine cavity. In most cases, endometriosis occurs in the pelvic region, for example, in the ovary, Douglas space or sacro-uterine ligament. Rare cases of endometriosis can occur outside the pelvis in the peritoneum, urinary tract, gastrointestinal tract, nervous system, chest, subcutaneous tissue and skin. A new trend in the management of patients with endometriosis is accurate non-invasive diagnosis of the extent of the disease using modern imaging techniques, ultrasound and magnetic resonance imaging (MRI) [1]. Endometriosis is now considered to be a systemic disease rather than a disease predominantly affecting the pelvis, affecting metabolism in the liver and adipose tissue, leading to systemic inflammation, and altering gene expression in the brain causing sensitisation to pain and mood disorders [2,3]. Endometriosis has overall detrimental effects on women‘s functional status, their physical, psychological, social and sexual well-being [4–6]. The extent of endometriosis often does not correlate with subjective complaints, so in addition to the assessment of the extent and classification of the disease (according to the internationally accepted classification), it is appropriate to assess the quality of life of patients. Quality of life can be assessed and compared using structured interviews or validated questionnaires [7]. The quality of life of partners living with a woman with endometriosis is also known to be reduced. The aim of our study was to obtain information on the quality of life of women with endometriosis aged 18–30 years by using the Endometriosis Health Profile-30 (EHP-30) questionnaire.
Materials and methods
For the use of the Czech version of the EHP-30 questionnaire, we obtained a license from Oxford University. The questionnaire was completed by women aged 18–30 years who had a confirmed diagnosis of endometriosis and were not pregnant at the time of completion of the questionnaire or in the past. Data were collected from 10 February 2023 to 8 October 2023 using the online platform Click4survey. Prior to running the actual EHP-30 questionnaire, respondents were asked a series of questions that classified them according to set criteria. A total of 184 women who met the entry criteria were classified for our subsequent evaluation. For our subsequent evaluation, a total of 184 women who met the entry criteria were classified. The questionnaires were distributed via social networks Facebook and Instagram, through the patient organisation ENDOtalks and the REHASPRING centre (accredited by the Ministry of Health of the Czech Republic). Through the questionnaires, we wanted to find out the common features and impact on the quality of life of women.
Results
The EHP-30 questionnaire was completed by 184 women (Tab. 1) and the group of women was divided into age categories (Tab. 2). The questionnaire was evaluated according to the guidelines for its evaluation (Tab. 3). The Kruskal-Wallis test for multiple independent samples was used to obtain the results (Tab. 4) and Spearman‘s correlation coefficient was used to measure the order dependence of the traits of the variables of interest (Tab. 5).
When divided into age categories, the age category 27–30 years was the most represented. A quarter of women were aged 24–26 years, more than a tenth were aged 21–23 years and only six women were aged 18–20 years (Tab. 2).
The aggregate EHP-30 index for all women averaged 57.0 points with a standard deviation of 20.43 points. The range of summary index scores for women was from 0 to 97.5 points (no woman reached the maximum possible score of 100), so the best score was 0 and the worst was 97.5 points. The median, the middle value of the ordered set by size, was 59.3 points. The modus, the most frequent value, was 0. Thus, women most often had a total of 0, but this is only because of the large range of possible variations in the total score (different values of the summary index for each woman), with no other number more numerous than 0, and yet there were only four such women (Tab. 3).
We predicted that the Pain domain would have the greatest impact on the quality of life of women with endometriosis, but the highest mean score was found for the Control and Powerlessness domain at 66.4 points, less for Social Support at 58.4 points, followed by Emotional Well-being at 58.2 points, even less for the Pain domain at 51.3 points, and the last domain was Self-Image at 50.7 points (Tab. 3).
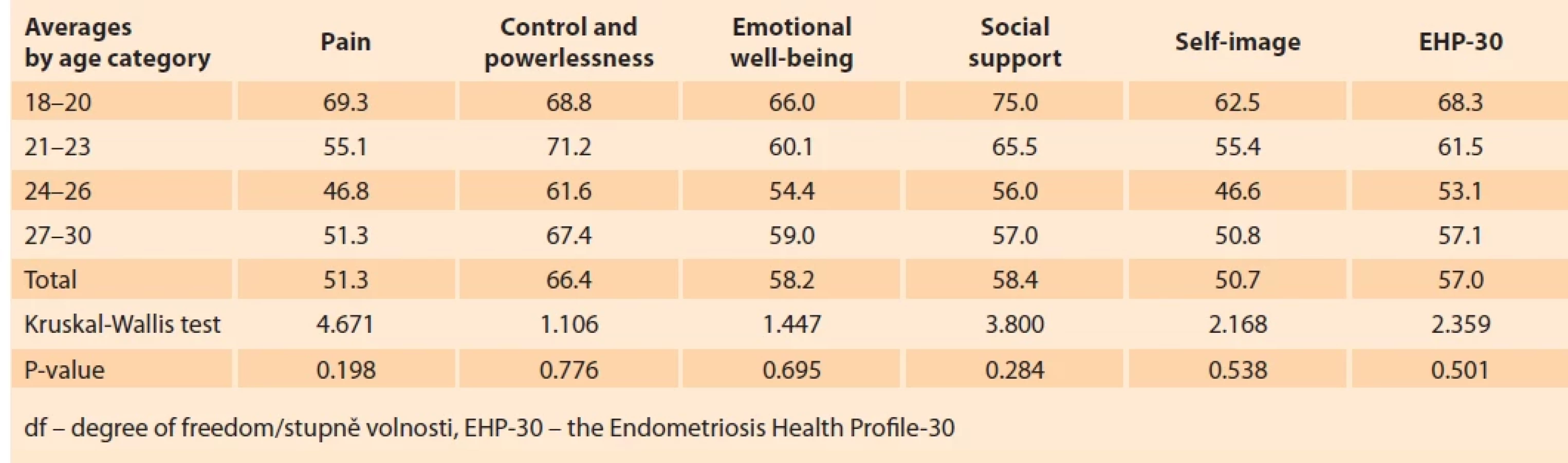
The above results showed that pain does not affect the quality of life of women with endometriosis the most. Women rated the questions related to the Control and Powerlessness domain the lowest. We hypothesised that the importance of pain on the quality of life of women with endometriosis would increase with increasing age. The mean values of each dimension and index are shown in Tab. 4. The 24–26 age category shows the smallest average values (best results) for all domains and the index. On the other hand, the 18–20 age category shows the highest average values (worst results) for almost all domains and for the index, except for the Control and Powerlessness domain, where the 21–23 age category has the highest average (Tab. 4).
However, according to the Kruskal--Wallis test, these differences between age categories are not statistically significantly different for any of the dimensions or the index. Thus, age does not statistically significantly affect the EHP-30 index or its individual domains. The above results showed that the perception of pain does not increase with increasing age, on the contrary, the youngest women in the age category 18–20 years perceive pain the worst.
The values of the correlation coefficient are shown in Tab. 5. There is a very strong positive correlation between the EHP-30 index and each domain, strongest between the domains Control and Powerlessness (0.833), and Pain (0.811), slightly weaker with the remaining domains. The domains also have a positive correlation with each other, the highest – and very strong – being Pain and Control and Powerlessness (0.769). The Self-Image domain has only a weaker positive correlation with the other domains (coefficient values between 0.434 and 0.488). The other domains have a moderately strong positive correlation with each other (coefficient values between 0.543 and 0.601).
All these correlations are statistically significant and are moderate to very strong. The individual domains are statistically significantly positively correlated with each other and with the EHP-30 index.




Discussion
Based on our assumptions, we expected that the majority of women surveyed would be between the ages of 27 and 30 due to a diagnosis of endometriosis. Since the condition for inclusion of women in the study was confirmed endometriosis. This hypothesis was formulated on the basis of a study by Hudelist et al. that was conducted in Austria and Germany, countries with similar health systems to the Czech Republic [8]. The results of the study show that the average time from the onset of symptoms to confirmation of a diagnosis of endometriosis was 10.4 years, and 74% of women received at least one misdiagnosis during this time [8]. Analysis of our data confirmed this alternative hypothesis, showing that women aged 27–30 years made up the largest proportion of our sample (59.2%). On the contrary, younger age groups (18–20 years, 21–23 years) were less represented in our sample (3.3% and 12.5%, resp.). This agreement with our hypothesis suggests that delays in the diagnosis of endometriosis may be a common phenomenon in the context of the Czech Republic and similar countries with similar health systems. A study by Palaščáková Špringrová et al. on screening of pelvic floor muscle function and the prevalence of dysmenorrhea in women in the Czech Republic showed that of the 362 women included in the study, 53% had insufficient information about endometriosis, were unaware of its symptoms and consequences, and dysmenorrhea, a common symptom of endometriosis, was present in almost half of the women, mostly nulliparous women (74%) [9]. In our study, we hypothesised that pain would have the greatest impact on the quality of life of women with endometriosis. This was based on a study by Facchin et al. in which 110 patients with surgically diagnosed endometriosis (78 with pelvic pain and 32 without pain symptoms) and 61 healthy controls completed two psychometric tests assessing quality of life, anxiety and depression [10]. Participants reported the intensity of four types of pain (dysmenorrhoea, dyspareunia, non-menstrual pelvic pain and dyschezia) on a numerical scale. Patients with endometriosis with pelvic pain had poorer quality of life and mental health compared to patients with asymptomatic endometriosis and healthy controls [10]. However, our study shows that the lowest rated domain was Control and Powerlessness with an index of 66.4. Pain with an index of 51.3 was only the 4th lowest rated domain. The results confirm that factors associated with feelings of control and powerlessness have a greater impact on women‘s quality of life than pain itself. In their study, Janoušková et al. assessed the quality of life of women with endometriosis 3 months before and 3 months after the start of endometriosis treatment with the EHP-30 questionnaire [11]. When comparing the quality of life with the EHP-30 questionnaire, significantly better quality of life scores were found in the Control and Powerlessness, Emotional Well-being and Pain domains at 3 months after treatment initiation, and their data indicate that endometriosis affects several aspects of quality of life in patients with this disease [11]. Our study also found that Social Support (58.4) and Emotional Well-being (58.2) also have a relatively high index. We can speculate that lack of social support and emotional well-being plays a significant role in women‘s perceptions of quality of life. This finding is important for designing interventions and support measures aimed at improving the quality of life of women with endometriosis. Our results are supported by the research of Calvi et al. who found a negative impact of chronic inflammatory disease endometriosis on social functioning and interpersonal relationships [12]. This research highlights the importance of providing social support and adequate care for women suffering from endometriosis or similar health problems [12]. Overall, our study shows that pain is not the only factor affecting the quality of life of women with endometriosis. Control and powerlessness, lack of social support and emotional well-being are important factors that should be taken into account when designing interventions and support measures to improve women‘s quality of life. Furthermore, we expected that women of older age would rate pain-related questions worse. This hypothesis was based on a paper by Wang et al. suggesting that recent molecular genetic findings on endometriosis and the normal endometrium may lead to a modified model where reactive epithelial progenitor or stem cells after menstruation may be found outside the uterus [13]. Based on these findings, we hypothesized that with each subsequent menstrual period, the disease worsens and thus the pain level. However, our analysis using the Kruskal-Wallis test did not confirm our results Tab. 4. The effect of pain on the quality of life of women with endometriosis was rated worst by women aged 18–20 years and best by women aged 24–26 years. This inconsistency with our assumption suggests that there is no direct correlation between pain perception and age or extent of disease. Based on these results, we suggest that the factors influencing pain perception and the extent of endometriosis may be more complex than anticipated. Perhaps age is not the only determining factor, but other variables such as individual pain sensitivity or the complexity of endometriosis may play a role. These results suggest the need for further research to identify these factors and their influence on pain perception in women with endometriosis.
Conclusion
The results of the study are important not only for medical practice, but also to support education and awareness programs aimed at increasing endometriosis awareness among physicians and the public. Early diagnosis can contribute to a more controlled and effective treatment plan, which can significantly improve the quality of life of women affected by this disease. We have tried to emphasise the importance of collaboration between different medical disciplines in providing care for patients with endometriosis. A comprehensive approach that includes gynaecologists, physiotherapists, psychologists and other specialists can significantly improve the quality of care and life for women with this diagnosis. In this study, we investigated the impact of endometriosis on women’s quality of life. One of the main findings of this paper is that many women with endometriosis suffer not only from physical pain associated with menstruation, but also from psychosocial difficulties that significantly affect their daily lives and relationships. These findings highlight the importance of a multidisciplinary approach to endometriosis treatment, which includes not only medical care but also psychological support and social counselling.
Zdroje
1. Indrielle-Kelly T, Frühauf F, Burgetová A e tal. Diagnosis of endometriosis 1st part – overview of diagnostic approaches. Ceska Gynekol 2019; 84 (4): 252–259.
2. Tian Y, Pei K, Bai J et al. Primary perineal endometriosis – a case report and literature review Ceska Gynekol 2024; 89 (1): 40–43. doi: 10.48095/cccg202440.
3. Hugh ST, Kotlyar AM, Flores VA. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. Lancet 2021; 397 (10276): 839–852. doi: 10.1016/S0140-6736 (21) 00389-5.
4. Buster JE. Managing female sexual dysfunction. Fert Steril 2013; 100 (4): 905–915. doi: 10.1016/j.fertnstert2013.08.026.
5. Montanari G, Di Donato N, Benfenati A et al. Deep infiltrating endometriosis: sexual satisfaction, desire, orgasm, and pelvic problem interference with sex. J Sex Med 2013; 10 (6): 1559–1566. doi: 10.1111/jsm12133.
6. Soliman AM, Yang H, Du EX et al. The direct and indirect costs associated with endometriosis: a systematic literature review. Hum Repord 2016; 31 (4): 712–722. doi: 10.1093/humrep/dev335.
7. Koliba P, Kužel D, Fanta M. Endometrióza a kvalita života. Ceska Gynekol 2017; 82 (5): 411–418.
8. Hudelist G, Fritzer N, Thomas A et al. Diagnostic delay for endometriosis in Austria and Germany: causes and possible consequences. Hum Reprod 2012; 27 (12): 3412–3416. doi: 10.1093/humrep/des316.
9. Palaščáková Špringrová I, Němec M, Fasselová V et al. Screening of pelvic floor muscle function and prevalence of dysmenorrhea in women. Rehabil Fyz Lek 2024; 31 (1): 4–10. doi: 10.48095/ccrhfl 20244.
10. Facchin F, Barbara G, Saita E et al. Impact of endometriosis on quality of life and mental health: pelvic pain makes the difference. J Psychosom Obstet Gynaecol 2015; 36 (4): 135–141. doi: 10.3109/0167482X.2015.1074173.
11. Janoušková K, Lemrová A, Ivanová K et al. Surgical and/or conservative treatment improves quality of life (EHP-30) in patients with endometriosis. Ceska Gynekol 2024; 89 (3): 188–194. doi: 10.48095/cccg2024188.
12. Calvi C, Sherman KA, Pham D. Loneliness and perceived social support in endometriosis: the roles of body image disturbance and anticipated stigma. Int J Behav Med 2024; 31 (3): 433–444. doi: 10.1007/s12529-023 - 10230-w.
13. Wang Y, Nicholes K, Shih IM. The origin and pathogenesis of endometriosis. Annu Rev Pathol 2020; 15 : 71–95. \doi: 10.1146/annurev - pathmechdis-012419-032654.
ORCID of authors
I. Palaščáková Špringrová 0009-0003-6851-6310
M. Němec 0000-0001 - 6871-7401
Submitted/Doručeno: 15. 3. 2025
Accepted/Přijato: 20. 5. 2025
PhDr. Ingrid Palaščáková Špringrová, Ph.D.
REHASPRING centrum s. r. o.
Krajní 2075
250 88 Čelákovice
palascakova@rehaspring.cz
Štítky
Dětská gynekologie Gynekologie a porodnictví Reprodukční medicínaČlánek vyšel v časopise
Česká gynekologie

2025 Číslo 5
Nejčtenější v tomto čísle
- Vaginal fisting and risk of anogenital injury
- Placental insufficiency and late-onset growth restriction in fetuses appropriate for gestational age
- Results of the Endometriosis Health Profile-30 questionnaire in women aged 18– 30 years in the Czech Republic
- Prevalence and hormonal profiling of secondary amenorrheic patients presenting to a fertility clinic – an observational study