
The association between 1st trimester serum kisspeptin level and antenatal complications
Souvislost mezi hladinou kisspeptinu v séru v I. trimestru a prenatálními komplikacemi
Cíl: Naším cílem bylo zhodnotit využitelnost hladiny kisspeptinu (KP) v séru, měřeného v I. trimestru (11–14 týdnu), jako nového biomarkeru, který může predikovat prenatální komplikace. Materiály a metody: Prospektivní případová kontrolní studie prospektivně shromážděných dat. Vzorky krve všech pacientek (n = 124) byly uchovány při –70 °C pro stanovení hladin KP-10 a KP-54 v séru. Byly stanoveny a srovnány hladiny KP u žen, u kterých došlo ke komplikacím vč. retardace růstu plodu (FGR – fetal growth retardation), těhotenstvím indukované hypertenze (PIH – pregnancy-induced hypertension), předčasného porodu, gestačního diabetu a úmrtí plodu. Kontrolní skupinu tvořily odpovídající subjekty, které dokončily těhotenství bez problémů. Byl zkoumán prediktivní účinek hladiny KP v séru na nepříznivé výsledky těhotenství. Výsledky: Mezi všemi pacientkami s nepříznivými výsledky těhotenství byla hladina KP-10 významně vyšší u těch, u kterých došlo k FGR (p = 0,025). V kohortě pacientek postižených těhotenstvím indukovanou hypertenzí (PIH), buď samotnou nebo doprovázenou preeklampsií, byla zaznamenána tendence k vyšším hladinám KP-10 (p = 0,059), ačkoli nebylo dosaženo statistické významnosti. Nicméně pokud jde o KP-10, vypočtená cutoff hodnota a plocha pod křivkou (AUC – area under the curve) pro predikci nástupu FGR byly statisticky významné (AUC: 0,684; p = 0,006). Bylo zjištěno, že model vytvořený s KP-10, PIH a plazmatickým proteinem A spojeným s těhotenstvím (PAPP-A) je významný při predikci vývoje FGR (p = 0,006; NPV: 98 %; PPV: 21,4 %; OR: 0,10; 95% CI 0,016–0,611). Závěry: Hladiny KP v séru matky v I. trimestru mohou být využity jako biomarker v I. trimestru, který může predikovat vývoj FGR.
Klíčová slova:
kisspeptin-10 – kisspeptin-54 – výsledek těhotenství – omezení růstu plodu – těhotenstvím indukovaná hypertenze
Authors:
Özlem Kayacık Günday 1
![]() ; Ayhan Vurmaz 2
; Ayhan Vurmaz 2
![]() ; Mehmet Yılmazer 1
; Mehmet Yılmazer 1
![]()
Authors‘ workplace:
Department of Obstetrics and Gynecology, Faculty of Medicine, Afyonkarahisar University of Health Sciences Afyonkarahisar, Turkey
1; Department of Biochemistry, Faculty of Medicine, Afyonkarahisar University of Health Sciences, Afyonkarahisar, Turkey
2
Published in:
Ceska Gynekol 2025; 90(3): 212-221
Category:
Original Article
doi:
https://doi.org/10.48095/cccg2025212
Overview
Objective: We aimed to evaluate the usefulness of serum kisspeptin (KP), measured in the 1st trimester (11–14 weeks), as a new biomarker that can predict antenatal complications. Materials and methods: A prospective case-control study of prospectively collected data. Blood samples of all patients (N = 124) were preserved at –70 °C for the assessment of serum KP-10 and KP-54 levels. The KP levels were analyzed for comparison among women who experienced complications including fetal growth retardation (FGR), pregnancy-induced hypertension (PIH), preterm delivery, gestational diabetes, and fetal death. The control group consisted of matching subjects who completed their pregnancies without problems. The predictive effect of serum KP on adverse pregnancy outcomes was investigated. Results: Among all adverse pregnancy outcomes, the KP-10 level was significantly higher in patients who developed FGR (P = 0.025). In the patient cohort affected by PIH, either accompanied by preeclampsia or standalone, there was a trend towards higher KP-10 levels (P = 0.059), although statistical significance was not achieved. However, regarding KP-10, the calculated cut-off value and the area under the curve (AUC) for predicting the onset of FGR were statistically significant (AUC: 0.684; P = 0.006). The model established with KP-10, PIH, and pregnancy associated plasma protein-A (PAPP-A) was found to be significant in predicting the development of FGR (P = 0.006; NPV: 98%; PPV: 21.4%; OR: 0.10; 95% CI 0.016–0.611). Conclusions: First trimester maternal serum KP levels may have the potential to be used as a 1st trimester biomarker that can predict the development of FGR.
Keywords:
fetal growth restriction – kisspeptin-10 – kisspeptin-54 – pregnancy outcome – pregnancy-induced hypertension
Introduction
Kisspeptin (KP) is a polypeptide consisting of 145 amino acids (aa), encoded by the KISS-1 gene and it was first identified as a human malignant melanoma metastasis suppressor [1]. Other KPs are formed by proteolysis of this polypeptide: 54 aa (KP-54; metastin), 14 aa (KP-14), 13 aa (KP-13), and 10 aa (KP-10). They bind to the KISS-1 receptor (KISS-1R; also known as GPR54) via a C-terminal region containing Arg-Phe-NH2 [2].
In recent years, it has become clear that both KISS-1 and KISS-1R are highly expressed in the early invasive placenta [2], are produced by trophoblast cells throughout pregnancy at increasingly higher circulating levels, and the major circulating isoform is KP-54 [3]. Notably, there is a significant increase in circulating KP-54 immunoreactivity from 1,230 pmol/L in the 1st trimester to 9,590 pmol/L in the 3rd trimester, which subsequently returns to non-pregnancy levels postpartum (8 pmol/L) [4]. Among all KPs, KP-10 has a major role in regulating trophoblast invasion. KP-10 exclusively triggers the release of intracellular calcium in early placental trophoblasts [5]. It has been shown that KP-10 reduces collagenase activity and dose-dependent matrix metalloproteinase-2 (MMP-2) activity, which causes a decrease in trophoblast migration but does not prevent proliferation [5]. It was also reported that KP-10 was separated from KP-54 before reaching the circulation and that it was the KP with the highest affinity for KISS-1R [6].
The hypothesis that KPs regulate trophoblast invasion during implantation has been proven by showing that KISS-1 and KISS-1R expression decreases in choriocarcinoma cells [7]. Again, the demonstration that KP/GPR-54 expression decreases in vitro in habitual abortion suggests that KP plays a role in the embryo implantation process [8]. It has also been reported that KP plays a role in immune regulation to prevent maternal-fetal rejection [9].
Evidence indicates that the placental-based KP/KISS-1R signaling systems play a regulatory role in pregnancy, as demonstrated in conditions like fetal growth restriction (FGR) and preeclampsia (PE), both of which are fundamentally associated with issues in placentation [10]. It has also been suggested that serum KP levels are associated not only with FGR, pregnancy-induced hypertension (PIH), and PE, but also with gestational diabetes (GDM) [11] and preterm birth (PTB) [12]. All of these findings may mean that KPs are involved in a complex process during pregnancy.
Antenatal complications are associated with acute and chronic maternal and fetal outcomes worldwide. Therefore, the search for a new, non-invasive, and useful marker that will enable early diagnosis continues intensively. KP has the potential to be such a marker. For this purpose, in our study, we planned to investigate whether 1st trimester KP levels have a place in predicting antenatal complications.

Materials and methodology
In this case-control study, 124 female patients between the ages of 18 and 35 years, who were admitted to a tertiary hospital for routine pregnancy control and had a pregnancy between 11 and 14 weeks between April 2022 and March 2023, were included. The study was approved by the Afyonkarahisar University of Health Sciences Clinical Research Medical Ethics Committee (No: 2022/514 and 2023/231) and conducted under the Helsinki Declaration on human subject research.
Exclusions were made for patients with multiple pregnancies, smoking habits, fetal anomalies, maternal infections, chronic diseases, malignancies, gestational trophoblastic disease, and ectopic pregnancy. Among the pregnant women included in the study, those who reached term without any antenatal complications formed the control group. Pregnant women with FGR, PIH and/or PE, PTB, GDM, and fetal death constituted the study group.
The gestational age was verified via 1st trimester ultrasound. Obstetric examination findings and laboratory results for all patients were documented. Patients received ongoing monitoring and treatment in accordance with international guidelines until delivery.
Antenatal complications
PIH is characterized by blood pressure readings of ≥ 140/90 mmHg on two separate occasions, at least 4 hours apart, occurring after the 20th week of pregnancy, following a previously normal blood pressure [13]. PIH can lead to complications such as PE. Aside from the requirement of blood pressure levels reaching ≥ 140/90 mmHg for diagnosing PE, singleton pregnant women meeting the subsequent criteria were enrolled in the study group: glomerular endotheliosis, proteinuria (≥ 300 mg/day of protein or protein/creatinine ratio ≥ 30 mg/mmoL), or any other indications of organ dysfunction. Two subtypes of PE have been defined: early (< 34 weeks’ gestation) and late (≥ 34 weeks’ gestation) onset PE [14].
FGR included individuals with estimated fetal weight below the tenth percentile for gestational age, alongside abnormal umbilical artery Doppler findings (such as a pulsatility index exceeding the 95th percentile and/or the presence of reverse diastolic flow or loss of diastolic flow [15].
PTB encompassed women who delivered after 24 weeks but before 37 weeks of gestation, either due to spontaneous onset or preterm premature rupture of membranes [16].
To diagnose GDM, patients underwent an oral glucose tolerance test after 20 weeks of gestation, where a fasting plasma glucose level of ≥ 5.6 mmol/L or a glucose level of ≥ 7.8 mmol/L two hours after ingesting 75 g of glucose indicated GDM [17].
All patients were requested to undergo a double screening test at 11–14 weeks of gestation. Simultaneously, approximately 10 mL of blood was collected into biochemistry tubes containing ethylenediaminetetraacetic acid (10 mg/mL blood) for serum KP-10 and KP-54. These samples were then stored at –70 °C until analysis, with serum KP analyses conducted at the end of the study upon completion of sample collection. Serum KP-10 and 54 were tested by an enzyme-linked immunosorbent assay (ELISA, BT LAB, Shanghai Korain Biotech Co., Ltd., China) using a commercially available kit according to the manufacturer’s instructions (run at 450 nm with a Thermo Scientific Multiskan FC Microplate [Thermo Fisher Scientific Instruments Co. Ltd. Shanghai/China] reader). Results are expressed as ng/mL.
Statistical analysis
Continuous variables were described using mean and standard deviation (SD), while categorical variables were expressed as proportions and percentages of the total. Spearman correlation analysis was conducted to assess the relationship between KP levels and pregnancy/birth variables, age, hemoglobin, aspartate aminotransferase (AST), and body mass index (BMI). To determine the KP cut-off value and its predictive accuracy for FGR, receiver operating characteristic (ROC) analysis was employed, and the area under the ROC curve was calculated. MedCalc software (Medcalc Software, Ghent, Belgium) was utilized for these analyses. For the significant KP-10 cut-off value identified, patients were stratified into two groups: group 1 (< 1.75) and group 2 (≥ 1.75). Continuous variables between these groups were compared using either Student’s t-test or Mann-Whitney U-test based on the distribution’s normality, while categorical variables were compared using Pearson’s chi-square or Fisher’s exact test. Logistic regression analysis was employed to assess the significance of the established model for FGR and KP-10, followed by sensitivity and specificity analyses. Statistical analysis was conducted using the Statistical Program for Social Sciences v.23.0 (SPSS, Chicago, IL, USA) with a significance level set at P ≤ 0.05 for all tests.
Results
Demographic and pregnancy characteristics of 124 pregnant patients included in the study (mean ± SD) were as follows: age: 28.2 ± 5.65 (years); BMI: 25.55 ± 4.7 (kg/m2), Hb: 12.43 ± 1.23 (g/L), gestational age at the time of blood sampling: 12.53 ± 0.82 (weeks), NT: 1.35 ± 0.37 (mm), PAPP-A: 1.16 ± 0.57 (MoM), week of birth: 37.84 ± 3.54 (weeks), and baby weight at birth: 3,089 ± 474.52 (g). Fifty-six patients (45.2%) had a vaginal birth at term, and 66 patients (53.2%) had a cesarean section. Ninety patients did not develop any complications during pregnancy, while one (0.8%) had curettage due to abortion, eight (6.5%) had fetal death, seven (5.6 %) had PIH (with or without PE), 6 (4.8%) had preterm delivery (with or without PPROM), GDM was present in four (3.2%), FGR (without PIH) was present in four (3.2%), and amniotic fluid pathology was present in four (3.2%) patients; overall, a total of 34 patients had antenatal complications. There was no difference between patients with and without antenatal complications in terms of age, BMI, birth weight, hemoglobin (Hb), leukocytes, AST, and parity (P > 0.005) (Tab. 1).
KP-10 level was found to be significantly higher in patients who developed FGR (group with FGR: 2.17 ± 0.84, non-FGR group: 1.82 ± 1.11; P = 0.025). KP-10 level was higher in patients with PIH ± PE, although the result was not significant (in patients with PIH ± PE, 2.59 ± 1.38 vs. 1.81 ± 1.05, P = 0.059) (Tab. 2). The results for KP-54 were not significant (P > 0.05). In the ROC analysis, the KP-10 cut-off value and AUC predicting the likelihood of developing FGR were significant (AUC: 0.684; P = 0.006; KP-10 : 1.749; Youden index J: 0.4052, 95% CI 0.594–0.764) (Fig. 1). In 79 patients (group 1), the maternal serum KP-10 value was below 1.75 ng/mL, whereas in 45 patients (group 2), it was 1.75 ng/mL or higher. Group 2 exhibited a significantly higher number of patients with FGR and PIH with or without PE compared to Group 1 (P = 0.004; 0.026, resp.) (Tab. 3). A noteworthy positive correlation was found between KP-10 and KP-54. However, no correlation was observed between KP-10 and patient age, maternal BMI, blood count parameters, gestational week, PAPP-A MoM value, and infant birth weight (P > 0.05) (Tab. 4). For the effect of KP-10 level on the development of FGR, the model established with PIH ± PE, Hb level, and PAPP-A parameters was significant (P = 0.006) (Tab. 5). In the model, while KP-10, Hb, and PAPP-A alone were not significant, the FGR risk increase with PIH ± PE was significant (NPV: 98%; PPV: 21.4%; OR: 0.10; 95% CI 0.016–0.611) (Tab. 5).
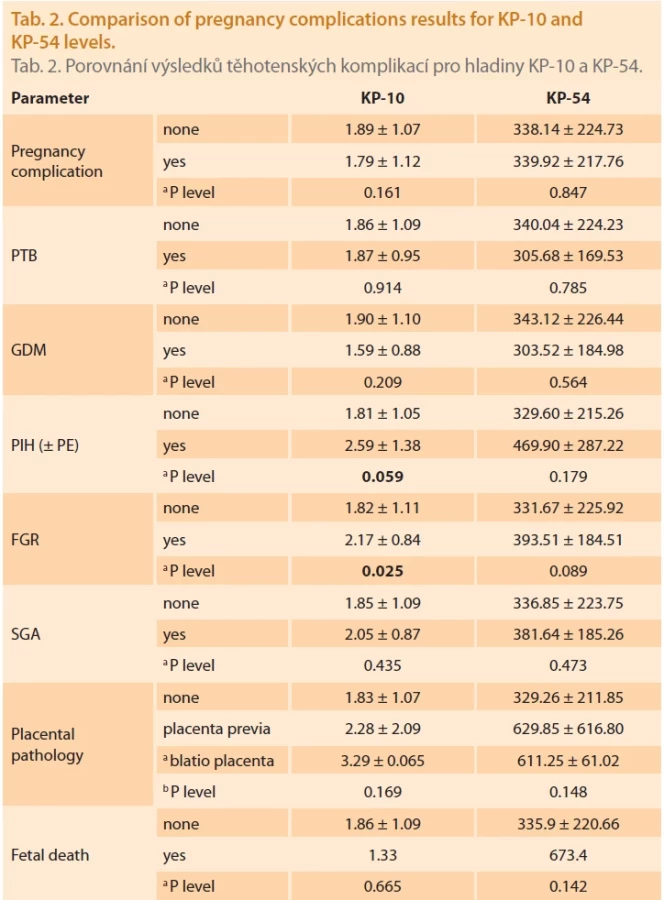
a Mann-Whitney U-test or b Kruskal-Wallis test for diff erences between KP-10 and KP-54 levels.
FGR – fetal growth retardation/zpomalení růstu plodu, GDM – gestational diabetes mellitus/gestační diabetes mellitus, KP – kisspeptin, PE – preeclampsia/preeklampsie, PIH – pregnancy-induced hypertension/těhotenstvím indukovaná hypertenze, PTB – preterm birth/předčasný porod, SGA – small for gestational age/malý na gestační věk


a Mann-Whitney U-test or b Student’s T-test for diff erences between normal and elevated KP-10 groups.
c Pearson Chi-Square.
d Fisher’ s Exact Test.
AST – aspartate aminotransferase/aspartátaminotransferáza, BMI – body mass index/index tělesné hmotnosti, FGR – fetal growth retardation/zpomalení růstu plodu, hCG – human chorionic gonadotropin/lidský choriový gonadotropin, KP – kisspeptin, N – number/počet, PAPP-A – pregnancy associated plasma protein-A/plazmatický protein-A spojený s těhotenstvím, PIH – pregnancy-induced hypertension/těhotenstvím indukovaná hypertenze, SD – standard deviation/směrodatná odchylka


Discussion
In our study, the KP-10 level of patients who developed FGR was significantly higher than that of healthy pregnant women, and the predictive effect of KP-10 for FGR was significant together with the development of PIH rather than alone. There was no difference in serum KP-10 and KP-54 levels between patients with antenatal complications and healthy pregnant women. Furthermore, there were no disparities between the two groups regarding clinical and demographic factors such as age, BMI, and parity. Upon reviewing the literature, it becomes evident that kisspeptins (KPs) have been extensively investigated in patients with PE. In addition to examining the association between KPs and PE, research has also delved into their relevance to FGR. Numerous studies have reported decreased levels of kisspeptins in cases of FGR compared to uncomplicated pregnancies [10,18]. Abbara et al. [10] examined both FGR and PE in their study and found the KP levels of women with PE and FGR to be lower than those with only PE, but higher than those of women with only FGR (P = 0.0004). In contrast to our findings, previous studies have reported significantly lower plasma levels of kisspeptins (KPs) in pregnancies complicated by FGR both at the end of the 1st trimester (9–13 weeks) and in the 3rd trimester (28–40 weeks) compared to pregnancies in the control group. Although various maternal and environmental factors have been proposed to contribute to the pathogenesis of FGR, impaired uteroplacental perfusion resulting from abnormal trophoblast invasion and inadequate remodeling of spiral arteries, which limits oxygen supply to the placenta, plays a crucial role. This ischemic insult leads to the generation of reactive oxygen radicals, and ultimately apoptosis, contributing to the development of FGR [19]. Based on this information, the researchers argued that low circulating KP levels reflected low placental mass in FGR. In studies where the KP level was measured in early pregnancy, it may not be appropriate to explain the results only with this effect. Contrary to studies arguing that it decreases, Ibanoğlu et al. found the median serum KP level in the patient group with late-onset FGR to be significantly higher than in the control group (79.4 vs. 39.8 pg/mL; P = 0.001) [20].
In today’s conditions, it does not seem possible to diagnose and prevent FGR before the symptoms appear. In clinical practice, it can be said that the most commonly used method for the early diagnosis of FGR is the uterine artery Doppler, but its sensitivity in predicting FGR is very low [21]. In recent years, there have been reports suggesting that microRNAs (miRNAs) could serve as potential biomarkers for predicting or diagnosing pregnancy complications [22]. However, the practical utility of these tests is limited by their costliness. The situation does not seem to be much different for PE. Diagnosis is usually made late after the disease appears. Although many markers have been studied to predict the development of PE, no reliable marker other than sFlt-1 and sEng has been identified [23]. Currently, the most common screening tool used for PE risk is the Doppler ultrasound analysis, which has low predictive value [24]. Therefore, it is important to find more useful biomarkers with high sensitivity and specificity for FGR and PE. KP has, therefore, become a remarkable marker. However, in studies conducted, there are conflicting results regarding the circulating KP level for PE, similar to FGR. Early studies showed lower plasma or serum KP levels in women with PE. Madazli et al. [25] found significantly lower levels of KP-54 in the 1st trimester maternal serum of women with PE compared to the control group. Armstrong et al. [18] reported that between the 16th and 20th weeks of pregnancy, KP levels in women who later developed PE were significantly lower than in controls. These findings were inconsistent with the proposed role of KP in inhibiting trophoblast invasion. Some researchers associated this finding with the size of the placenta and argued that a small placenta, which is frequently observed especially in EOPE patients, leads to lower KP levels [3]. Later studies showed that preeclamptic women exhibited elevated plasma [10] or serum [26,27] levels of KP compared with healthy women. In a recent study, Fang et al. revealed that both serum and placental KISS-1 levels were upregulated in patients with PE and they reported that KISS-1 may be an autocrine/paracrine factor that locally regulates trophoblast invasion [26]. Again, Ibanoğlu et al. also found that the KP level was significantly higher in late-onset PE (LOPE) patients than in the control group [28]. Unlike these studies, Nijher et al. did not find a significant difference in plasma KP concentrations between hypertensive pregnant women and normotensive pregnant controls [29]. Interpreting conflicting results poses challenges due to the incomplete understanding of the pathophysiology underlying hypertensive disorders in pregnancy, particularly those stemming from PE. PE exhibits diverse etiologies depending on its onset timing, thus it should not be perceived as a singular disease manifesting across different pregnancy stages [30]. While the EOPE phenotype is associated with impaired placental development and FGR, the LOPE phenotype is more associated with endothelial dysfunction [14].
Research involving protein and expression analysis has been conducted to elucidate the involvement of KP in pregnancy. In an intriguing study on KP expression, researchers observed a circadian rhythm in KISS-1 expression during term pregnancies, characterized by peaks at 4 : 00 a. m. and 12 : 00 p. m. [31]. A similar situation may apply to circulating KP levels. In our study and almost all other studies, the hours during which patients were sampled were not taken into account. In addition, the reason for the different results may be due to different measurement methods used for KP, the fact that some measurements were performed in serum and some in plasma, the fact that some authors measured total KP concentration while others studied only a single KP isoform, and the lack of standardization in laboratory tests. As a biomarker, studying KP in serum is more sensitive, and the tests used here are more stable [32]. Accordingly, it may be advantageous to investigate serum values for KP in our study.
In our hypertensive pregnant group, all patients who developed PE were LOPE, and since the pregnant women with PIH and without PE reached term, very low birth weight and small placenta were not out of the question. In addition to abnormal placentation, immune dysregulation and maternal inflammatory response have been shown to play a role in the pathogenesis of PIH, and recent research suggests that genetic factors, environmental factors, and epigenetic modifications play a role together [33].
The fact that there was a more heterogeneous hypertensive patient group than the pure PE group may also have affected our results. The type of KP and the week of maternal blood sample collection were widely distributed across studies (8, 12, 14, 16, and 20 weeks) and were not standardized across studies. In our study, the average week for blood sampling was 12.5 weeks.
Interestingly, it has been suggested that KP is a regulator of vascular tone that may induce the development of maternal hypertension [34]. KISS-1R expression has been detected in maternal smooth muscles, aorta and coronary arteries, and umbilical cord [35]. Also, angiogenesis inhibition and vasoconstriction effects of KP-10 have been observed [36]. These findings suggest that KP may play a role in the pathogenesis of LOPE by affecting vascular tone, as well as its effect on placentation in EOPE, and may be an explanation for the high KP results in the development of LOPE, as in our study. Here, the significant cut-off value for KP-10 predicting FGR was 1.75 ng/mL. There were significantly more FGR and PIH patients above this value. Additionally, the FGR predictive effect of KP-10 was significant when evaluated together with PIH. The development of immune tolerance mechanisms that prevent syncytiotrophoblast rejection during implantation is also important for a successful pregnancy. Although the antimetastatic function of KP during pregnancy is more emphasized, the fact that immunologic functions such as inhibiting cytotoxic reactions, supporting Th2-type response, and increasing the population of T regulatory cells have also been demonstrated [31]. These findings may be taken into consideration in explaining the contradictory results.
When the literature is examined, studies on the relationship between GDM and KP are insufficient, and the results are contradictory. It was reported that placental KISS-1 and KISS-1R expression increased in pregnant women with GDM in the 3rd trimester [11], plasma KP levels were lower than controls [37], and in another study, similar to our study, no difference was observed [38]. It has been reported that placental expression of KP increases significantly in women with PTB compared to those who give birth at term [12], but no change in circulating KP was observed [12]. Abbara et al. found plasma KP levels to be higher in pregnant women who performed PTB (P = 0.014). In our study, there was no significant difference in KP-10 and KP-54 levels between those who were monitored for PTB and pregnant women who gave birth at term. Qiao et al. showed that KISS-1 expression was increased in the placenta of patients with PE with intrauterine death and birth asphyxia compared to normal newborns, and they argued that abnormal upregulation of KISS-1 expression may contribute to the underlying mechanism of birth asphyxia [39]. In our study, there was no significant relationship between fetal death and serum KP.
The reason for the many conflicting results put forward for the relationship of KP with antenatal complications may be the rather complex interactions between KISS-1 signaling in the brain, pancreas, liver adipose tissue, and placenta [40]. These interactions need to be clarified through more comprehensive studies.

Conclusion
As a result, in our study, KP-10 was significantly higher in pregnant women with FGR, and there were significantly more pregnant women with FGR and PIH above the threshold value. Overall, given that there is no conclusive evidence showing that circulating KP levels consistently decrease or increase during antenatal complications, our study contributes to our understanding of the role of KP in antenatal complications. Also, the prospective design of our study and the fact that two separate KP isoforms were studied in serum in all patients simultaneously are its strengths. However, our study has some limitations. First, the patient population is relatively small. In addition, the times at which patients were sampled were not taken into account, and the circadian rhythm observed in KISS-1 expression [31] may also affect the results, as it may also be relevant for circulating KP. Although our study suggests that KP-10 has the potential to be used as a 1st trimester marker to predict the development of FGR, especially in association with PIH, prospective cohort studies that are comprehensive prospective cohort studies are needed.
Sources
Labels
Paediatric gynaecology Gynaecology and obstetrics Reproduction medicineArticle was published in
Czech Gynaecology

2025 Issue 3
Most read in this issue
- Effectiveness of physiotherapy on pain relief and functional recovery post-cesarean section
- Analysing risk factors for foetal growth outcomes – the influence of maternal conditions and congenital cytomegalovirus infection
- Robson’s classification – a way to reduce the number of caesarean sections?
- Gastroschisis – current options for prenatal diagnosis and subsequent management