
Effectiveness of physiotherapy on pain relief and functional recovery post-cesarean section
Účinnost fyzioterapie na úlevu od bolesti a funkční zotavení po císařském řezu
Úvod: Počty císařských řezů (CS – cesarean section) celosvětově rostou, přičemž související poporodní komplikace jsou výrazně vyšší ve srovnání s vaginálním porodem. Řešení těchto komplikací pomocí optimalizovaného managementu a cílené fyzioterapie je klíčové pro zlepšení mateřských výsledků a kvality života. Cíl: Cílem této studie bylo zhodnotit účinnost fyzioterapie na úlevu od bolesti a obnovení funkční aktivity žen po CS. Materiál a metody: Do studie bylo zapojeno 91 pacientek, které byly přijaty do porodnické nemocnice pro elektivní CS. Kontrolní skupině (47 žen) byl poskytnut standardní předoperační a pooperační dohled. Intervenční skupina (44 pacientů) kromě standardní péče absolvovala fyzioterapii, která zahrnovala předoperační péči (fyzioterapeutický výcvik, edukační výcvik) a pooperační cvičení (dechové, oběhové a pánevní cvičení spolu s masáží pojiva). Výsledky po CS byly analyzovány po dobu 3 dnů. Výsledky: Nižší intenzita pooperačních bolestí a snazší chůze od 1. dne, nižší obtížnost při provádění funkčních činností 2. den (snazší otočení na lůžku a přechod do sedu), rychlejší obnova střevní motility v důsledku průchodu flatusu za 3,5 hod a defekace na 10 hod, snížená potřeba analgetik navíc 4,21krát (OR = 0,24; 95% CI 0,10–0,58; p = 0,02) a bylo zjištěno významné snížení doby trvání hospitalizace (OR = 0,24; 95% CI 0,09–0,57; p = 0,02). Závěr: Studie prokázala účinnost navrženého fyzioterapeutického programu v časném období po CS ve smyslu snížení bolesti a zlepšení obnovy funkční aktivity organizmu.
Klíčová slova:
císařský řez – fyzioterapie – porodnická rehabilitace – fyzioterapeutická edukace – syndrom pooperační bolesti
Authors:
Svitlana Ostafiichuk 1
![]() ; Nataliia Drohomyretska 1
; Nataliia Drohomyretska 1
![]() ; Olena Kusa 1
; Olena Kusa 1
![]() ; Oksana Zhukuliak 1
; Oksana Zhukuliak 1
![]() ; Olha Neiko 1
; Olha Neiko 1
![]() ; Taras Kotyk 2
; Taras Kotyk 2
![]()
Authors‘ workplace:
Department of Obstetrics and Gynecology, Ivano-Frankivsk National Medical University, Ivano-Frankivsk, Ukraine
1; Department of Human Anatomy, Ivano-Frankivsk National Medical University, Ivano-Frankivsk, Ukraine
2
Published in:
Ceska Gynekol 2025; 90(3): 204-211
Category:
Original Article
doi:
https://doi.org/10.48095/cccg2025204
Overview
Background: Cesarean section (CS) rates are rising globally, with associated postpartum complications significantly higher compared to vaginal delivery. Addressing these complications through optimized management and targeted physiotherapy is crucial for improving maternal outcomes and quality of life. Objective: This study aimed to evaluate the effectiveness of physiotherapy on pain relief and restoration of functional activity in women after CS. Material and methods: 91 patients, who were admitted to an obstetric hospital for elective CS, were involved in the study. The control group (47 women) received standard pre - and postoperative supervision. The intervention group (44 patients), in addition to standard care, underwent physiotherapy, which included preoperative care (physiotherapy training, educational training), and postoperative exercises (breathing, circulation, and pelvic exercises, along with connective tissue massage). The results were analyzed after CS for 3 days. Results: A lower intensity of postoperative pain and easier walking from the 1st day, a lower level of difficulty in performing functional activities on the 2nd day (easier turning in bed and transition to a sitting position), faster recovery of intestinal motility due to the passage of flatus in 3.5 hours and the act of defecation after 10.0 hours, decreased requirement of extra analgesics by 4.21-fold (OR = 0.24; 95% CI 0.10–0.58; P = 0.02), and a significant reduction in the length of hospital stay (OR = 0.24; 95% CI 0.09–0.57; P = 0.02) were established. Conclusion: The study revealed the effectiveness of the proposed physiotherapy program in the early post-cesarean period in terms of reducing pain and improving restoration of the body’s functional activity.
Keywords:
Physiotherapy – cesarean section – obstetric rehabilitation – physiotherapy education – post-operative pain syndrome
Introduction
Cesarean section (CS) is one of the most common operations in obstetrics [1]. The frequency of CS is increasing rapidly all over the world [2]. During the period from 2015 to 2020, the frequency of CS in Ukraine has increased by 26.3% [3], reaching 26.7% of the total amount of labors in 2021 [4].
Comparison between CS and vaginal delivery has indicated a higher frequency of postpartum complications following CS [5]. The levels of maternal mortality and postpartum infection after CS are higher than in vaginal delivery [6]. Additionally, Duran et al. concluded that women experienced more pain, breastfeeding problems, decreased sleep quality and comfort, anxiety, delayed functional activity, and prolonged postpartum hospitalization after CS [7]. Pain, mobilization difficulties, challenges in personal hygiene, breastfeeding issues, and emotional changes have been identified as the most significant problems in women after CS [8]. Sis Çelik et al. (2020) demonstrated the association between the type of anesthesia and delivery method with difficulties in daily activities, pain intensity, newborn care, maintaining personal hygiene, urination, defecation, and passage of flatus [9]. Moreover, difficulties in the postoperative period have a significant negative impact on the mental well-being and quality of life of women [10].
Nowadays, it is postulated that optimizing the management of women during pregnancy and the post-CS period, along with evidence-based regular physical activity, plays a crucial role in improving the quality of life of mothers [11,12]. In this context, prenatal education plays an important role in pregnancy and labor outcomes [13].
Breathing exercises have demonstrated a significant impact on the quality of the recovery in the post-operation period [14], reducing pain and anxiety [15]. Circulation exercises as part of physiotherapy to reduce edema, accelerate recovery after the anesthetics, improve blood circulation, and prepare patients for the effort required to get out of bed [16]. Slow motility of the gastrointestinal system in the postoperative period causes bloating, nausea, vomiting, and pain, which negatively affects the comfort level of patients [17,18]. Connective tissue massage is one of the conservative methods for intestinal stimulation in the treatment of constipation [19], menstrual pain relief in primary dysmenorrhea, the frequency of menstrual cycle disorders, reduction in depression [20], and post-CS recovery [21].
There have been various studies examining the impact of physiotherapy on post-CS recovery [21–25]; however, these studies differ significantly in the type of training provided, the combination of proposed exercises, and duration of observation. This study aims to evaluate the effect of preoperative training and a comprehensive physiotherapy program (breathing, circulation, and pelvic exercises, along with connective tissue massage) on the dynamics of pain relief, reduction of challenges in daily activities, recovery of intestinal motility, and the need for additional analgesics. Additionally, the impact of these interventions on the length of hospital stay will be assessed.
Materials and methods
Study design and participants
This study was conducted at the City Clinical Perinatal Center in Ivano-Frankivsk, Ukraine, during July 2023 to June 2024. The research was approved by the Ethics Committee of the Ivano-Frankivsk National Medical University (protocol No. 119/21 dated February 24, 2021) and conducted according to the Declaration of Helsinki ”Ethical Principles of Medical Research Involving Human Subjects.” All of the women signed the ”Informed consent to participate in the study.”
The study included 100 patients aged 22 to 38 years who were admitted for elective CS. The inclusion criteria were systemically healthy women and indications for elective CS. The exclusion criteria were:
- two or more surgical interventions on the abdominal and pelvic organs in the anamnesis including CS;
- severe extragenital pathology, obstetric complications;
- maternal complications during and after CS;
- diastasis recti abdominal muscles greater than 2 cm;
- general anesthesia.
Participants were involved in the study according to eligibility criteria based on medical records and pregnancy history, and they were divided into two equal groups before elective CS. The control group received pre - and postoperative supervision according to standard protocols [3]. The intervention group, in addition to the standard pre - and post-CS care, underwent physical rehabilitation exercises.
Nine were excluded from the study due to complications after CS. The final sample size of the intervention group was 44 participants; the control group consisted of 47 participants.
Sample size
A priori power analysis was conducted using G*Power 3.1 to determine the minimum sample size required for the study. Based on an effect size of 0.8, a power of 0.8, and an alpha level of 0.05, the analysis revealed that a minimum of 30 participants per group would be necessary.
Interventions
Before labor, all women had standard psycho-prophylactic training and conscious parenting training.
CS protocol
All women underwent CS at full-term pregnancy (39 [39–40] weeks) in the City Clinical Perinatal Center, Ivano-Frnakivsk, Ukraine, via a Pfannenstiel laparotomy in the lower uterine segment by transverse incision, by suturing the wound on the uterus with a two-layer continuous vicryl suture according to the standard technique [3]. Immediately after surgery, all women were prescribed intravenous paracetamol (1,000 mg in 100 mL), and in the first 24 hours, parenteral administration of non-steroidal anti-inflammatory drugs was given as needed to control postoperative pain.
Physiotherapy
The first stage (pre-CS) started after hospitalization and included measures of preoperative care and physiotherapy training. During training, patients were instructed on how to correctly perform exercises after CS (breathing, circulation, and pelvic exercises, manipulations on connective tissue) [26–29]. During breathing exercises, special attention was paid to teaching women breathing movements during coughing by bending the legs at the knees and using a pillow to reduce pain. Circulation exercises were associated with flexion, extension, and rotation of the feet at the ankle joints, with exercises for bending and straightening the legs at the knees. Pelvic floor muscle exercises included long squeezes and short, quick squeezes. Patients aimed to work the muscles until they became tired and did the exercises regularly to help the muscles become stronger and more effective. Connective tissue manipulations involved interventions on the lumbosacral, lower thoracic, scapular, interscapular, and cervical areas.
The second stage was initialized after CS. Breathing and circulation exercises were started immediately after the patient was transferred to the postoperative care ward after the patient was awake and continued for 5–10 min every hour every day. Pelvic exercises were performed three times a day for 5–10 exercises daily and were recommended to be continued at home for up to 6–8 weeks. Manipulations on the connective tissue were performed daily for 15–20 min, and it was also recommended to continue up to 4 weeks after discharge from the hospital with a physiotherapist.
Outcomes
The results were analyzed for 3 days post-CS. Visual analog scale [30] was used to assess pain (0–10; 0 – no pain, 10 – unbearable pain) and functional activity (turning in bed, transitioning to a sitting position, walking) scores (0 – no difficulties, 10 – the impossibility of performing the activity) were assessed daily. Restoration of intestinal motility was assessed as the first time passing flatus and the independent act of defecation (hours after the operation). The requirement of extra analgesics (in addition to the standard care protocol) and the length of hospital stay due to maternal indications were measured.
Statistical methods
Statistical analysis has been performed in R v.4.0. The normality of data was assessed with the Shapiro-Wilk test. The descriptive statistic is provided as the median and interquartile range (IQR). Differences between independent variables were assessed with the Mann--Whitney U-test. Dependent variables were compared with the Kruskal-Wallis H-test with further post-hoc analysis (Bonferroni adjustment). Effect sizes (R-rstatix) were categorized as follows: small 0.1–0.3; moderate 0.3–0.5; and large > 0.5. Categorical data are provided as absolute numbers and frequencies, with further assessment with the Chi-Square test. Binary regression analysis was performed to investigate the association between performance of rehabilitation activities and risk of extended hospital stay. P value < 0.05 was accepted as significant.
Results
The intervention and control groups did not differ in terms of anthropometric data, obstetric anamnesis, and indications for CS (Tab. 1).
Daily analysis of the intensity of pain and difficulties of physical activities revealed significant improvement in the intervention group from a longitudinal perspective (Tab. 2). At the same time, the control group did not show rapid reduction and was higher than in the patient group. There were no differences in the difficulty of transitioning to a sitting position on the 1st day and turning in bed on the 1st and 3rd days (P > 0.05). A significant improvement in walking was found in the intervention group already from the 1st day.
After applying rehabilitation activities, there was a significant reduction in the time of restoration of intestinal motility (P < 0.001) (Tab. 3). A significant difference in the length of hospital stay between the intervention group and controls was established (P < 0.001). Also, the percentage of women staying in the hospital for more than 4 days was lower in the patient group compared to the controls (40.9 vs. 74.5%; P = 0.002).
A significant association between the requirement of extra analgesics and rehabilitation interventions was revealed during observation (Fig. 1, Tab. 3) by releasing pain intensity (Tab. 2). Implementation of the physiotherapy program reduces the chances of requiring extra analgesics by 4.21-fold (OR = 0.24; 95% CI 0.10–0.58; P = 0.02).
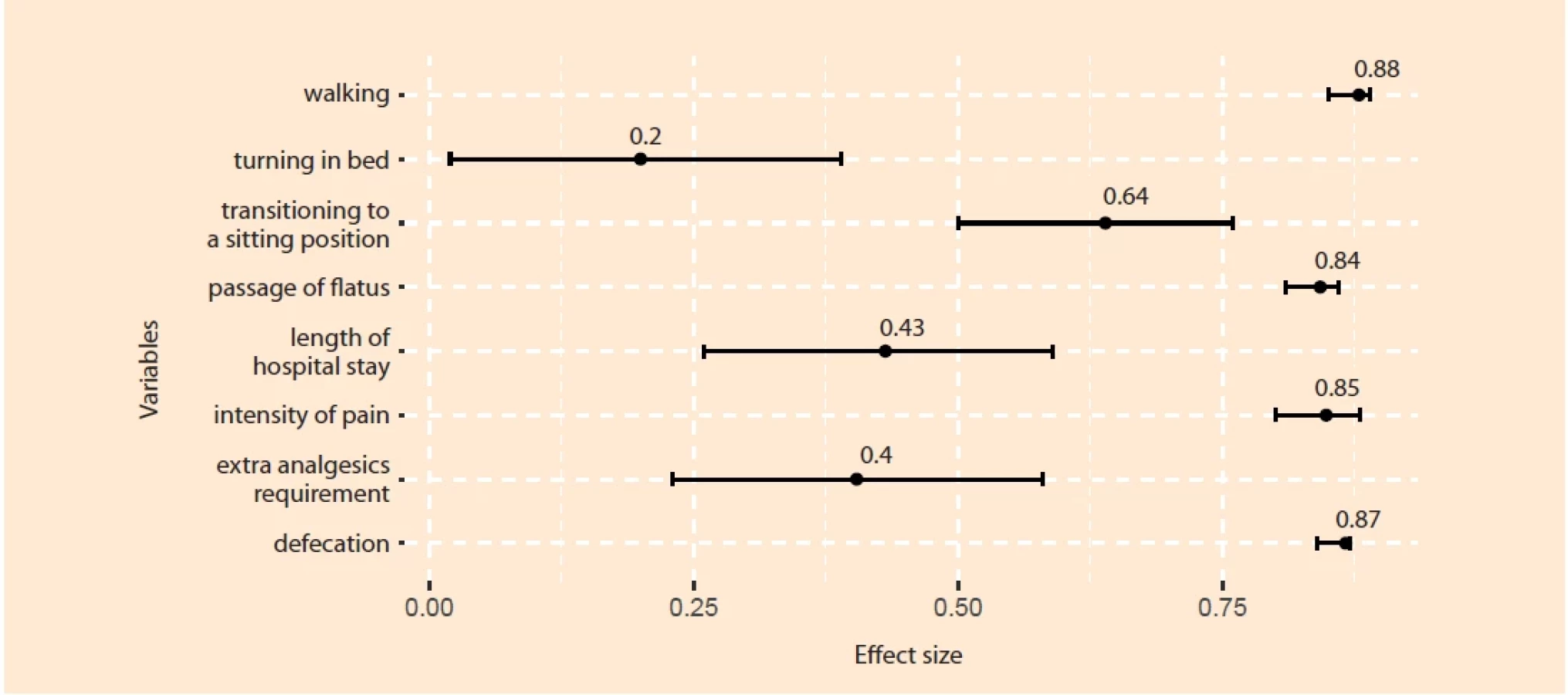
The physiotherapy exercises had a large effect on pain intensity, transitioning to a sitting position, walking, and intestinal motility (Fig. 2), and a moderate effect on the need for extra analgesics and length of hospital stay.
Results of the binary regression analysis demonstrated a significantly reduced probability of extended length of hospital stay after incorporating rehabilitation sessions in post-operative management (Tab. 4).





Discussion
The study’s findings revealed a positive impact of rehabilitation activities on the post-CS period. The rehabilitation program included training before the operation and physical activities (exercises to improve circulation, breathing, pelvic floor muscle exercises, connective tissue manipulation), which were performed for 3 days post-CS. As a result of applying the aforementioned rehabilitation, significant pain relief, accelerated physical rehabilitation, and decreased length of hospital stay have been achieved.
In our study, the intensity of pain significantly gradually decreased during the observation period in the intervention group. On the other hand, in the control group, pain relief wasn’t observed within the first two days of monitoring, and only on the third day it was significantly reduced, but its severity remained two-fold higher than in the study group. Similar findings were found by Weerasinghe et al. [24] and Ain et al. [22]. However, these studies cover only 2 days of post--cesarean monitoring. Moreover, the decreasing requirement for extra analgesics was observed, which was caused by the mitigation of pain in the intervention group as a result of applying rehabilitation activities [31]. This also included breathing exercises suppressing the sympathetic system and increasing the tone of the parasympathetic system, decreasing cortisol levels, leading to pain relief, and increasing concentration and a sense of tranquility [32]. Surprisingly, in the study by Weerasinghe et al. [24], the need for additional analgesics in both groups was higher despite lower values of pain intensity, compared to our study. It can be explained by differences in study groups, rehabilitation programs, personal perception of pain, and analgesics used.
Difficulties in daily activities (turning in bed, sitting, walking) were significantly progressively reduced daily along with faster restoration of intestinal motility in the intervention group. It should be noted that challenges with repositioning in bed and sitting up were similar in both groups on the first day. However, in the control group, significant improvement was observed only on the last day of the study, but did not reach the level of the intervention group except for turning in bed. Different postnatal exercise techniques reduce irritability and stress, decrease muscle tension, and aid in relaxation [33]. Moreover, lower back or pelvic pain is frequently observed after CS, and pelvic exercises substantially contribute to alleviating pain [34], which as a result may lead to improvement of daily activities. Additionally, physical activities positively influence the cardiovascular system and aerobic capacity [35]. Severe difficulties in turning in bed in short-term observation (8 hours after CS) despite applying a rehabilitation program were noted by Ali et al. [25] and can be caused by anesthesia and analgesia. At the same time, the authors concluded that rehabilitation exercises are effective in the early stages. This aligns with our findings, which show significant differences in walking difficulties, despite the high severity of these challenges in both groups on the first day after CS. Similarly to our results, significant improvement in daily activities on the background of rehabilitation sessions after post-CS has been also observed in a few studies [22–24,36].
In the present study, it was shown that the restoration of intestinal motility occurred faster in women in the intervention group. The passage of flatus and defecation – indicators of intestinal activity – based on the influence of various programs have been previously noted. The incorporation of a complex of pelvic floor muscle exercises and connective tissue massage in the sacral and lumbar regions, which was highlighted in the study of Çıtak Karakaya et al., played a role in the early onset of bowel function activity in the intervention group. Additionally, expedited initiation of daily activities (such as walking) may potentially lead to the restoration of intestinal motility [37].
The findings revealed a significant probability reduction in the length of hospital stay in the patient group after incorporating the proposed set of rehabilitation activities (4 [4–5] vs 5 [4.5–6] days; OR = 0.24 [0.09; 0.57]), which align with Weerasinghe et al. [13]. The percentage of patients, who required extended hospital stay, was significantly higher among participants with traditional post-CS care (74.5 vs 40.9%; P = 0.002). Such results allow achievement of a positive economic effect and reduce financial burden [38].
The generalizability of these results is subject to certain limitations. The study was from a single-center and involved a relatively small number of participants. Results of the study should be taken with caution for patients who are not within the eligibility criteria used in this study. Additionally, routine pre - and post-CS care has been performed according to national guidelines. Results of the study do not cover long-term outcomes and do not explore the effects of particular exercises included in a comprehensive physiotherapy program.
In conclusion, this study evaluated the impact of a comprehensive preoperative training and physiotherapy program, including breathing, circulation, pelvic exercises, and connective tissue massage, on postpartum outcomes following CS. The findings demonstrate that patients undergoing physiotherapy experienced significant improvements in pain relief (effect size = 0.85; 95% CI 0.80–0.88) and daily activities (effect size for turning in bed: 0.20; 95% CI 0.02–0.39; sitting: 0.64; 95% CI 0.50–0.76; walking: 0.88; 95% CI 0.85–0.89). Additionally, the physiotherapy program significantly improved intestinal motility (effect size for the passage of flatus: 0.84; 95% CI 0.81–0.86; defecation: 0.87; 95% CI 0.84–0.87), reduced the need for additional analgesics (OR = 0.24; 95% CI 0.10–0.58; effect size = 0.40; 95% CI 0.23–0.58), and shortened the length of hospital stay (OR = 0.24; 95% CI 0.09–0.57; effect size = 0.43; 95% CI 0.26–0.59). These results underscore the effectiveness of the physiotherapy program in enhancing postoperative recovery, highlighting its potential as a valuable component of post-CS care.
Sources
Labels
Paediatric gynaecology Gynaecology and obstetrics Reproduction medicineArticle was published in
Czech Gynaecology

2025 Issue 3
Most read in this issue
- Effectiveness of physiotherapy on pain relief and functional recovery post-cesarean section
- Analysing risk factors for foetal growth outcomes – the influence of maternal conditions and congenital cytomegalovirus infection
- Robson’s classification – a way to reduce the number of caesarean sections?
- Gastroschisis – current options for prenatal diagnosis and subsequent management