
Trisomy 16 mimicking hydatidiform mole
Trizómia chromozómu 16 mimikujúca hydatidóznu molu
Autori prezentujú prípad I. trimestrového potratu s klinicky suponovanou skorou formou kompletnej moly hydatidózy. Histopatologická a imunohistochemická analýza vylúčila kompletnú molu, ale histomorfologický profil naznačoval parciálnu hydatidóznu molu. Genetická analýza vylúčila parciálnu molu na základe biparentálnej kompozície genómu, ďalšie genetické analýzy odhalili trizómiu chromozómu 16. Trizómia chromozómu 16 je častou príčinou potratov v I. trimestri a môže viesť k vysoko abnormálnej histomorfológii placenty napodobňujúcej parciálnu molu. Genetické analýzy sú v týchto prípadoch rozhodujúce pre správnu diferenciálnu dia gnostiku, a teda pre stanovenie adekvátnej dispenzárnej starostlivosti a prognózy pre ďalšie gravidity.
Klíčová slova:
analýza DNA – trizómia 16 – aneuploidia – histomorfológia placenty
Authors:
Lajos Gergely 1,2
![]() ; Miroslav Korbeľ 2,3
; Miroslav Korbeľ 2,3
![]() ; Ľudovít Danihel 2,4; Vanda Repiská 1,2
; Ľudovít Danihel 2,4; Vanda Repiská 1,2
![]() ; Miroslav Tomka 1
; Miroslav Tomka 1
![]() ; Liam McCullough 2,3
; Liam McCullough 2,3
![]() ; Petra Priščáková 1,2
; Petra Priščáková 1,2
![]()
Authors place of work:
Institute of Medical Biology, Genetics and Clinical Genetics, Faculty of Medicine, Comenius University Bratislava, Bratislava, Slovak Republic
1; Centre for Gestational Trophoblastic Dis ease of Slovak Republic, Bratislava, Slovak Republic
2; 1st Department of Gynaecology and Obstetrics, Faculty of Medicine, Comenius University Bratislava, Bratislava, Slovak Republic
3; Institute of Pathological Anatomy, Faculty of Medicine, Comenius University Bratislava, Bratislava, Slovak Republic
4
Published in the journal:
Ceska Gynekol 2024; 89(5): 396-399
Category:
Kazuistika
doi:
https://doi.org/10.48095/cccg2024396
Summary
The authors present a case of 1st trimester miscarriage where an early, complete hydatidiform mole was clinically suspected. Histopathological and immunohistochemical analyses excluded a complete mole, but the histomorphological profile was in concordance with a partial hydatidiform mole. Genetic analysis excluded a partial mole based on biparental genome composition, where further genetic analyses detected trisomy of chromosome 16. Trisomy of chromosome 16 is a frequent cause of 1st trimester abortions and may lead to highly abnormal placental histomorphology mimicking a partial mole. Genetic analyses are crucial for proper differential diagnosis and for the determination of adequate follow-up and prognosis for further pregnancies.
Keywords:
DNA analysis – Aneuploidy – trisomy 16 – placental histomorphology
Introduction
Lethal chromosomal abnormalities, as a result of random aberrations of gametogenesis or fertilization, represent the dominant cause of pregnancy losses in the 1st trimester (aneuploidies and polyploidies incompatible with higher stages of intrauterine development). Among aneuploidies, trisomy of chromosome 16 is found most frequently [1,2].
Early molar pregnancies, especially partial moles, are difficult to dia gnose based on ultrasound and histopathological examination alone. Trisomy gestations may potentially display histomorphological features similar to partial moles [3,4].
We present a case of an early pregnancy loss, where an early complete hydatidiform mole was suspected based on ultrasound features and human chorionic gonadotropin (hCG) levels. The histomorphological profile was highly susceptible for a partial hydatidiform mole, but eventually the DNA analysis detected trisomy of chromosome 16.
Case presentation
A 33-year old primigravid patient was initially dia gnosed with suspected an early, complete hydatidiform mole at the 7th week of pregnancy, based on sonographic features and an abnormally elevated serum human chorionic gonadotropin (hCG) at 51,134 IU/l. Vacuum evacuation (D&E) of the uterine cavity was performed. The tissue evacuated from the uterine cavity was fixed in formalin for histopathologic and immunohistochemical analyses. The histopathological profile was consistent with a partial hydatidiform mole. Avascular, edematous, hydropic chorionic villi with a variable degree of trophoblast hyperplasia were detected (Fig. 1a). Groups of chorionic villi without morphological changes were also present. Positivity of p57 in the cytotrophoblast and mesenchymal stroma of chorionic villi excluded a complete hydatidiform mole (Fig. 1b). Genetic analysis was performed to confirm the dia gnosis of a partial mole.
DNA was isolated from microdissections of formalin-fixed paraffin-embedded chorionic villi and of the peripheral blood of the patient using QIAamp DNA FFPE Tissue Kit (QIAGEN) and DNeasy Blood & Tissue Kit (QIAGEN). Short tandem repeat (STR) genotyping was performed with a quantitative fluorescence polymerase chain reaction (QF-PCR) technique using the commercial kit GenePrint 10 System (Promega). Comparing STR alleles of the chorionic villi and of the patient, biparental genome composition was detected, which excluded the dia g – nosis of a partial mole. According to the Amelogenin locus (sex determining marker), the gonosomal complement of the product of conception was XY. Additionally, the DNA isolated from the chorionic villi was tested for aneuploidies of chromosomes 13, 15, 16, 18, 21, 22, X, and Y with a QF-PCR technique using the kit Devyser Extend v2 (Devyser). Physiologic number of chromosomes 13, 15, 18, 21, 22, gonosomal complement XY, and trisomy 16 were detected (Fig. 1c).
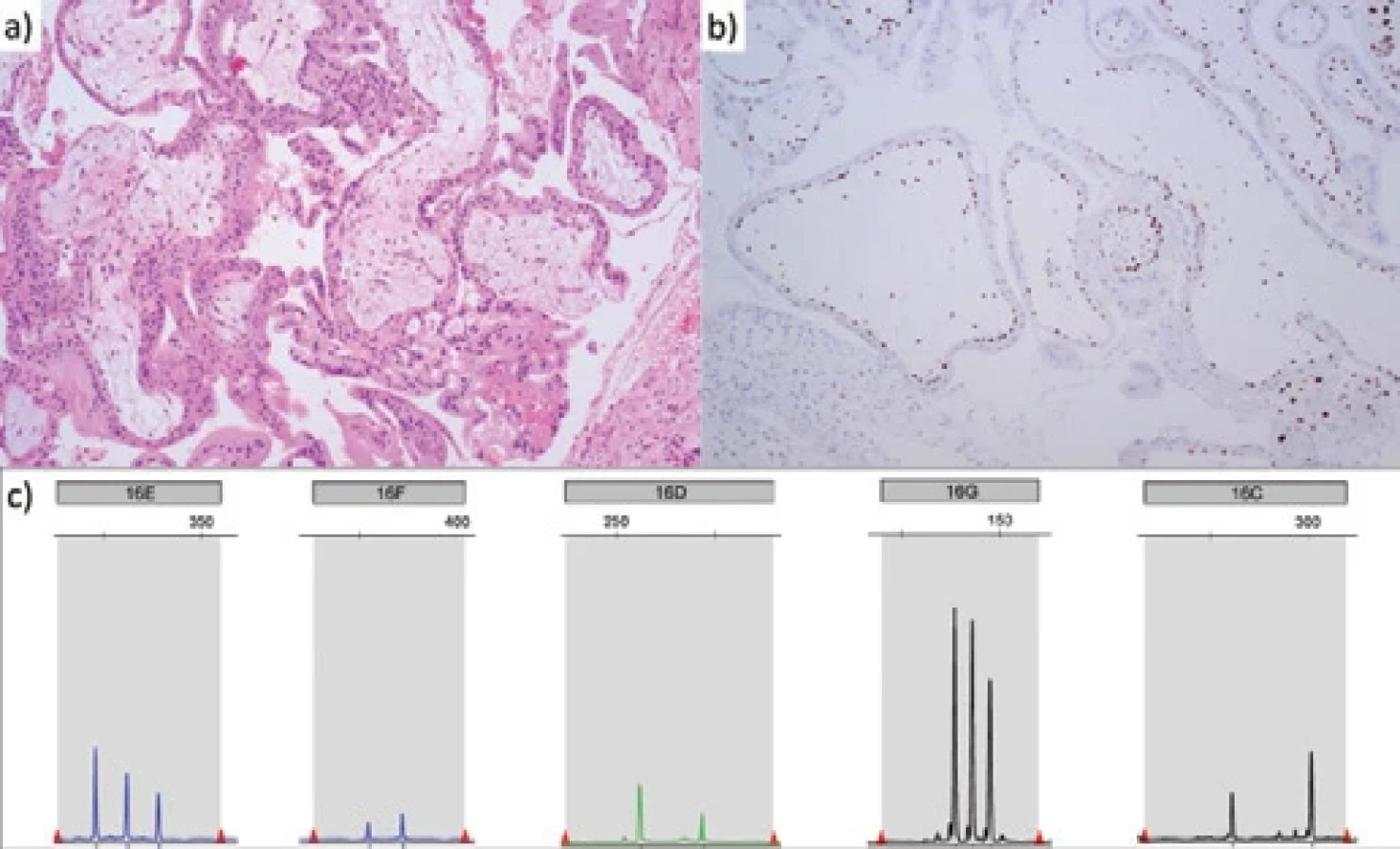
b) Positivity of p57 in the cytotrophoblast and mesenchymal stroma of chorionic villi excludes the diagnosis of a complete mole.
c) Trisomic allelic pattern of all chromosome 16 markers on QF-PCR electrophoretograms.
a) Avaskulárne, edematózne, hydropické choriové klky s rôznym stupňom hyperplázie trofoblastu (farbenie hematoxylínom a eozínom).
b) Pozitivita p57 v cytotrofoblaste a v mezenchymálnej stróme choriových klkov vylučuje diagnózu kompletnej moly.
c) Trizomický alelický vzor všetkých markerov chromozómu 16 na elektroforetogramoch QF-PCR.
Discussion
The histopathological profile of aneuploid pregnancies may include enlarged, scalloped chorionic villi, multifocal trophoblastic hyperplasia, stromal pseudo-inclusions, and decreased stromal vessels [5]. If the combination of these features is present, a DNA analysis may confirm or exclude diandric monogynic triploidy (eventually triandric monogynic tetraploidy) characteristic for partial hydatidiform moles. The vast majority of triploid partial moles arises due to dispermic fertilization (dispermic/heterozygous partial hydatidiform mole). Less frequently, the duplication of the sperm nuclear genome after fertilization can lead to a monospermic/ /homozygous partial hydatidiform mole. The gonosome complement is most often XXY. In approximately 2–3% of the cases, the partial mole has a tetraploid triandric monogynic genome composition as a result of trispermic fertilization [6–10].
The dominant cause of reproductive losses in the 1st trimester are lethal chromosomal abnormalities, including aneuploidies and polyploidies incompatible with higher stages of intrauterine development as a result of random aberrations of gametogenesis or fertilization [11]. Trisomy 16 represents approximately one third of all trisomies detected in miscarriages and all pregnancies with trisomy 16 result in 1st-trimester miscarriage, so the causal relationship between this genetic finding and the pregnancy loss in our patient is obvious [12]. Trisomy 16 is most likely the result of nondisjunction in maternal meiosis I and the risk of recurrence is probably negligible [13].
The length of chromosome 16 is 90,338,345 base pairs and it contains 863 coding genes [14]. For comparison, chromosome 21, whose trisomy is potentially viable is approximately half as long (46,709,983 base pairs) and contains approximately four times fewer coding genes (221) [15].
Although full trisomy 16 is incompatible with life, mosaic forms, concretely confined placental mosaicism and true fetal mosaicism occur in live births. The mosaic trisomy 16 cases are most probably caused by a meiotic chromosomal segregation error leading to a trisomic zygote and subsequent mitotic loss of the extra chromosome resulting in partial rescue of the aneuploidy. In contrast to true fetal mosaicism, the cell line with trisomy 16 is restricted to the placenta in confined placental mosaicism, while the fetal karyotype is normal. Confined placental mosaicism of chromosome 16 is associated with an 11-fold higher risk of delivering small-for-gestational-age (SGA) neonates, so we can presume impaired placental function in these cases [16,17].
True fetal mosaicism for trisomy 16 is associated with a 70% risk of congenital malformations, mostly heart defects. The risk of malformation possibly correlates to the level of mosaicism. The risk of developmental delay also correlates with the level of mosaicism and the presence of multiple malformations [17].
STR genotyping can help in the differential dia gnosis of partial moles, hydropic abortions, or abortions from other causes. Patient fol low-up is only indicated in cases of a partial mole due to increased risk of persistent gestational trophoblastic neoplasia. Patients with non-molar miscarriages do not require fol low-ups and are spared from unnecessary examinations and in postponing future pregnancy [6,8].
According to our experiences, formalin-fixed paraffin-embedded tissue samples are not ideal materials for molecular genetic studies – because of DNA fragmentation due to formalin fixation, QF-PCR with increased amount of input DNA often leads to informative results as in the presented case.
In the presented case, genetic analysis of products of conception first led to the exclusion of a partial hydatidiform mole (biparental genome composition), and secondly to the determination of the cause of miscarriage and abnormal villus morphology (trisomy 16).
Conclusion
Abortion caused by trisomy of chromosome 16 may clinically and histopathologically mimic a hydatidiform mole. At first, the exclusion of a complete hydatidiform mole using p57 immunohistochemistry is crucial. Additionally, a partial mole can be definitively confirmed/excluded by STR genotyping. To determine the cause of abortion with abnormal villous morphology, QF-PCR focused on the most common aneuploidies in reproductive losses (chromosomes 13, 15, 16, 18, 21, 22, X, and Y), which can be carried out even on formalin-fixed paraffin-embedded chorionic villi.
Zdroje
Štítky
Dětská gynekologie Gynekologie a porodnictví Reprodukční medicínaČlánek vyšel v časopise
Česká gynekologie

2024 Číslo 5
Nejčtenější v tomto čísle
- Intrahepatic cholestasis of pregnancy
- Spontaneous and post-interventional regression of cervical HPV infection
- Advantages of next-generation sequencing (NGS) in the molecular classifi cation of endometrial carcinomas – our experience with 270 cases
- Inherited thrombophilia and risk of venous thromboembolism in females in association with contraceptive use