
Epidemiological profile of pregnant women and perinatal outcomes of newborns with gastroschisis from a single reference center in Northeastern Brazil
Authors:
C. M. G. C. Escoto Esteche 1
![]() ; E. Araujo Júnior 1; B. C. Escoto Esteche 2
; E. Araujo Júnior 1; B. C. Escoto Esteche 2
![]() ; L. C. Rolo 1
; L. C. Rolo 1
![]()
Authors place of work:
Department of Obstetrics, Paulista School of Medicine – Federal University of São Paulo (EPM-UNIFESP), Sao Paulo, Brazil
1; Medical School, Christus University Center (UNICHRISTUS), Fortaleza, Brazil
2
Published in the journal:
Ceska Gynekol 2026; 91(1): 26-34
Category:
Původní práce
doi:
https://doi.org/10.48095/cccg202626
Summary
Objective: To determine the maternal epidemiological profile and perinatal outcomes of fetuses with gastroschisis at a reference center in Northeastern Brazil. Methods: A retrospective cohort study was conducted between January 2014 and December 2022 using medical records. Inclusion criteria comprised of pregnancies ≥ 24 weeks, with a prenatal diagnosis of gastroschisis confirmed in the postnatal period. Results: During the study period, 1,773 newborns with congenital anomalies were born at the service center, 50 were identified as having gastroschisis and four cases were excluded. Prevalence of gastroschisis was 11.5/10,000. Regarding the maternal sociodemographic profile, the mean age was 21 years, 38/46 (83%) were mixed, 34/46 (74%) had a partner, and 32/46 (70%) had high school education. Regarding associated maternal diseases, only 6/46 (13%) had hypertension, none had pre-existing diabetes mellitus, and 4/46 (8.7%) developed gestational diabetes mellitus. As for gastroschisis type, 33/46 (71%) were classified as simple, 11/46 (23.9%) as complex and 2/46 (4.4%) had no information. In 36/46 newborns with gastroschisis, primary closure was performed in the first surgery. The mean time of use of mechanical ventilation was 13 days, the mean time interval between surgery and ambient air was 8 days, the mean time of use of parenteral nutrition was 35 days, and the mean length of stay in the neonatal intensive care unit (NICU) was 39 days. Clinical complications in newborns with gastroschisis included neonatal infection in 35/46 (76%), blood transfusion in 33/46 (72%), hydroelectrolytic disorders and sepsis in 29/46 (63%), and cholestasis and fungal infection/sepsis in 8/46 (17%). Neonatal death occurred in 16/46 (34.8%). Conclusion: Newborns with gastroschisis presented high rates of surgery with primary closure, blood transfusion and neonatal infection. Furthermore, we identified prolonged use of parenteral nutrition, long stay in the NICU, and prolonged use of antibiotic therapy.
Keywords:
perinatal outcomes – prevalence – gastroschisis – epidemiological profile – reference center
Introduction
The incidence of abdominal wall defects is approximately 1 in 2,000 live births [1]. Gastroschisis is a congenital anomaly of the anterior abdominal wall, with the presence of herniated abdominal structures, most often the intestine and occasionally the bladder, stomach and liver. The defect is usually paraumbilical on the right, and the herniated organs do not have a protective membrane, remaining in direct contact with the amniotic fluid [2,3]. Gastroschisis is a rare malformation and has been addressed more frequently due to the discussion about its etiology, the increase in its incidence, the current possibility of earlier diagnosis of the malformation by ultrasound as well as, of course, advances in surgical techniques, with better nutritional support and postoperative care [4].
Increased incidence of gastroschisis in the UK had already been observed in 2006, particularly in younger women under the age of 20, where incidence was 4.71 per 10,000 compared with 0.26 per 10,000 in mothers over the age of 30 [5]. A study published in 2016 used data on gastroschisis from 15 US state programs to evaluate the average annual change in prevalence, comparing specific time periods (2006–2012 vs. 1995–2005). An increase of 30% was found, from 3.6/10,000 births in 1995–2005 to 4.9/10,000 births in 2006–2012 [6]. In Brazil, a study analyzed the annual incidence of gastroschisis from 2,000 to 2017 and identified the highest incidence in mothers under 20 years of age, which showed a significant increase during the study period [7].
Gastroschisis can be classified as simple or complex according to the conditions observed in the intestine. The simple form is the most common, with low morbidity and a better survival rate. On the other hand, the complex form is directly associated with prolonged hospital stay, short bowel syndrome, and death, with a high association with atresia, volvulus, necrosis, and perforation [8]. In Brazil, state of Rio de Janeiro, the mortality rate for isolated gastroschisis was 12.9% between 2005 and 2014 [9]. In the Brazilian global context of gastroschisis, only eight studies (most of the studies from the Southeast region) were found (912 patients), with mean maternal age of 20.7 years, mean antenatal diagnosis rate of 80.2%, mean cesarean section rate of 77.7%, mean hospital stay of 40.8 days, and mean mortality rate of 25.3% [10].
This study aimed to assess the maternal epidemiological data and perinatal outcomes of fetuses with gastroschisis at a reference center in northeastern Brazil.
Methods
A retrospective cohort study was conducted at the Assis Chateaubriand Maternity School, Federal University of Ceará (UFC), city of Fortaleza, sate of Ceará, Northeastern Brazil, between January 2014 and December 2022. The medical records of all fetuses with gastroschisis born at the service were carefully analyzed. Inclusion criteria comprised pregnancies ≥ 24 weeks, with a prenatal diagnosis of gastroschisis confirmed in the postnatal period by a neonatologist and/or pediatric surgeon. Exclusion criteria comprised absence of postnatal data and minor congenital anomaly. This study was approved by the UFC Research Ethics Committee.
We assessed the following maternal demographic characteristics: age; ethnicity; marital status; scholarship; and occupation. Obstetric characteristics included number of pregnancies, miscarriages, and deliveries, gestational age at the beginning of prenatal care, gestational age at diagnosis of gastroschisis, prenatal care at the service, number of ultrasound examinations at the service. Habits and maternal diseases included alcohol consumption, smoking, illicit drug use, body mass index (BMI), hypertension, pre-existing diabetes mellitus and gestational diabetes mellitus. Delivery and newborn data comprised delivery type, gestational age at delivery, sex, birth weight, and Apgar scores at the 1st and 5th minutes. Postnatal outcome surgery data were gastroschisis type, surgery type, time between birth and surgery, primary closure in the first surgery, surgical complications. Postnatal outcome data for neonatal intensive care unit (NICU) admission enclosed use of mechanical ventilation, use of continuous positive airway pressure (CPAP), time between surgery and ambient air, time on parenteral nutrition, time on antibiotic therapy, clinical complications, length of stay in NICU, death.
We collected and managed study data using the Research Electronic Data Capture (REDCap, Vanderbilt University, Nashville, TN, USA), an electronic data collection and management tool hosted at the UFC Clinical Research Unit. Variables were presented as mean and standard deviation, median, percentiles, minimum and maximum, frequency and prevalence. The Chi-square test of independence, Wilcoxon rank sum test and Fisher’s exact test were used to analyze participant characteristics, checking that the data did not follow a Gaussian distribution. Pearson’s Chi-squared test and Fisher’s exact test were used to investigate associations between categorical variables. A 5% significance level was used. Statistical analyses were performed using the R statistical program.
Resulst
During the study period, 1,773 newborns with congenital anomalies were born at the service and 50 were identified as having gastroschisis. Of these, three cases were excluded because of major malformations, and one case was excluded because of gestational age < 24 weeks. During the study period, we observed a variation in the annual prevalence of gastroschisis cases at the institution, ranging from 4.4–16.7/10,000 live births. During the nine years assessed (2014–2022), the prevalence of gastroschisis was 11.5/10,000.
In relation to maternal sociodemographic variables of the 46 pregnant women, we found that the mean age was 21 years (21.2 ± 4.6), 38/46 (83%) were mixed, 34/46 (74%) had a partner, 32/46 (70%) had high school education, and 24/46 (52%) did not have a paid occupation (Tab. 1).

(median).
Regarding obstetric characteristics, we found that the median number of pregnant women had a previous pregnancy without miscarriage and prenatal care started at 10 weeks of gestation. As for smoking and alcohol use, we found that 45/46 (98%) did not drink or smoke and 43/46 (96%) did not use illicit drugs. Regarding the BMI, we found that 22/46 (48%) had a BMI between 18.5 and 24.9 kg/m2. With respect to associated maternal diseases, we found that only 6/46 (13%) had hypertension, none had pre-existing diabetes mellitus, and 4/46 (8.7%) developed gestational diabetes mellitus (Tab. 2). The mean start of prenatal care was around the 12th week of pregnancy, and the diagnosis of gastroschisis was given around the 21st week of pregnancy. Regarding prenatal care at the institution, we found that 31/46 (67.4%) of patients came from the own institution and 38/46 (83%) of pregnant women had undergone an ultrasound at the institution.

BMI – body mass index
As for variables related to delivery, we found that 45/46 (98%) were delivered by cesarean section, the mean gestational age was 36 weeks, 23/46 (50%) were female, the mean birth weight was 2,315 grams, with 11/46 (23.9%) weighing < 2,000 grams, 19/46 (41.3%) weighing between 2,000 and 2,400 grams and 16/46 (34.8%) weighing > 2,500 grams. In terms of Apgar scores, we found that 27/46 (58.7%) had a score ≥ 8 at the 1st minute and 41/46 (89.1%) had a score ≥ 8 at the 5th minute. We found that 31/46 (67%) were born with appropriate weight for gestational age. Regarding the presence of associated anomalies, we found that 6/46 (13%) had some minor anomaly, with cryptorchidism being the most common (Tab. 3).

AGA – appropriate for gestational age, LGA – large for gestational age, SGA – small for gestational age
Concerning gastroschisis type, we found that 33/46 (71%) were classified as simple, 11/46 (23.9%) as complex and 2/46 (4.4%) had no information. Regarding the surgery, we found that 45/46 (98%) of newborns underwent some type of surgery. The mean time between delivery and surgery was 2.60 hours. In 36/46 newborns with gastroschisis, primary closure was performed in the first surgery. The mean time of use of mechanical ventilation was 13 days; the mean time interval between surgery and ambient air was 8 days; the mean time of use of parenteral nutrition was 35 days; and the mean length of stay in the NICU was 39 days. As for antibiotic therapy, we found that the mean was nearly four courses and the mean duration was 31 days (Tab. 4).

NICU – neonatal intensive care unit
Clinical complications in newborns with gastroschisis included neonatal infection in 35/46 (76%), blood transfusion in 33/46 (72%), hydroelectrolytic disorders and sepsis in 29/46 (63%), and cholestasis and fungal infection/sepsis in 8/46 (17%). Neonatal death occurred in 16/46 (34.8%) (Tab. 5).

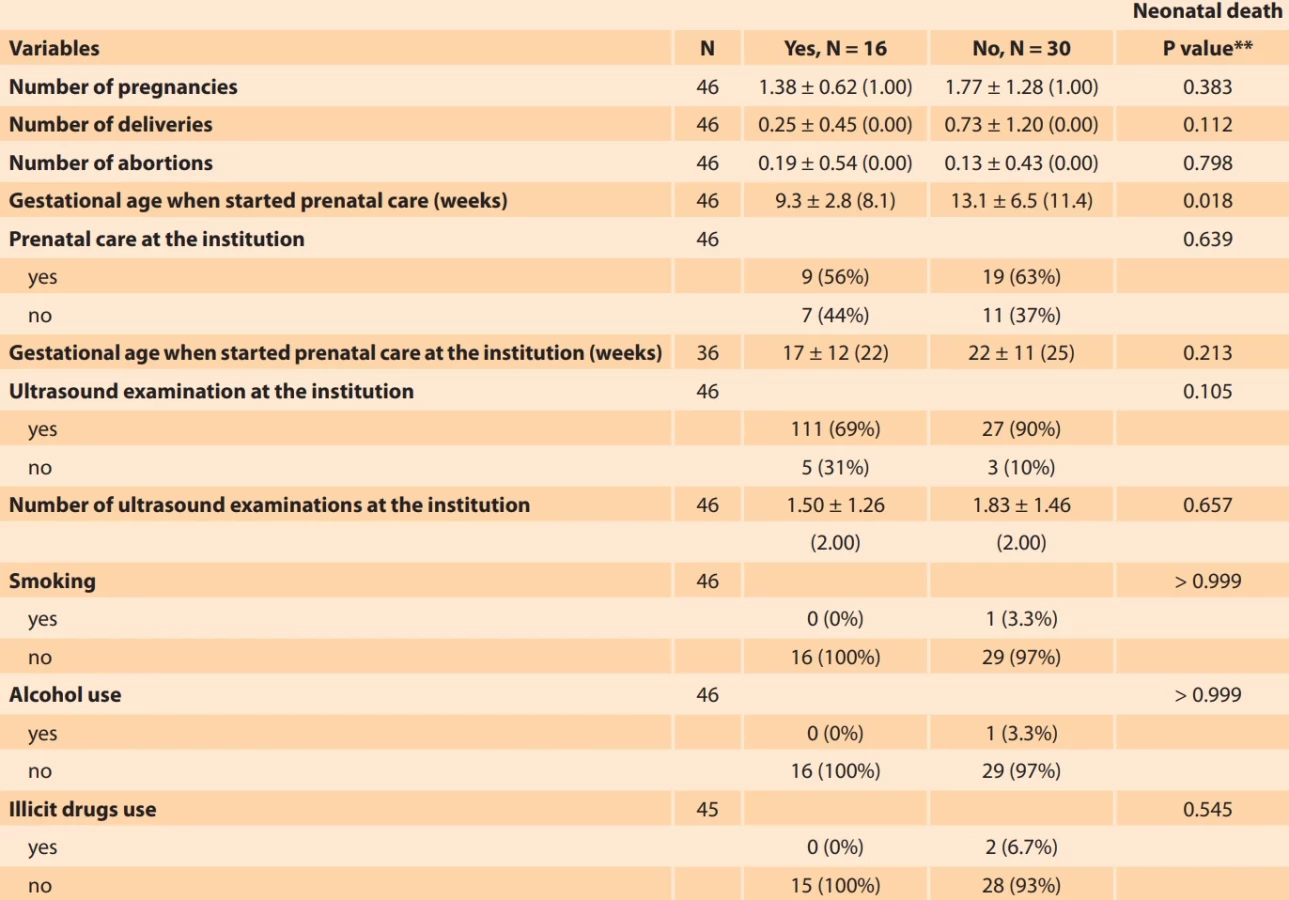
According to Tab. 6, in relation to the association between obstetric characteristics/maternal diseases and death of newborns with gastroschisis, only gestational age at the beginning of prenatal care showed a statistically significant association (P = 0.018). As for the association between surgical variables of newborns with gastroschisis, we observed that the following variables were associated with neonatal death: primary closure in the first surgery (P = 0.020); time of mechanical ventilation (P = 0.038); time of parenteral nutrition (P = 0.040); and length of stay in the NICU (P = 0.017) (Tab. 7). In the analysis of the association between clinical complications/gastroschisis type and death of newborns with gastroschisis, metabolic acidosis (P < 0.001) and gastroschisis type (P = 0.023) were statistically significant (Tab. 8).
BMI – body mass index

BMI – body mass index

NCIU – neonatal intensive care unit

Discussion
The prevalence of gastroschisis during the period assessed at our institution was 11.5/10,000 live births, data very similar to that presented by a university hospital center in Portugal between 2009 and 2019, with a prevalence of 10/10,000 [11]. In our study, we found a prevalence 10 times higher than that in Europe, which was 1.35 in 2021, including live births and stillbirths [12]. In a systematic review that included 10 articles between 1999 and 2022, the prevalence of gastroschisis in Sub-Saharan Africa varied widely, ranging from 0.026 to 1.75 [13]. In a recent study that estimated the prevalence of gastroschisis in all Brazilian regions, the overall prevalence of gastroschisis was 2.47 per 10,000 births, being higher in the Central-West region and lower in the Northeast region [14].
The median maternal age in our study was 21 years, which is similar to that found in the United States and Sub-Saharan Africa [13,15]. However, it differed from the findings in Japanese women living in Europe and the United States, where maternal age was predominantly between 30 and 39 years [16]. According to a study carried out by EUROCAT, the probable association between young maternal age and gastroschisis is due to the fact that this anomaly is caused by vascular rupture, in addition to younger mothers being more exposed to alcohol consumption, smoking and drug use [17]. However, although mean maternal age was young, we did not find a statistically significant association with these substances in our study because 98% of pregnant women did not use alcohol or tobacco and 96% did not use illicit drugs.
In this study, almost half of the pregnant women (48%) had a BMI within the normal range and only 8.7% had a BMI < 18.5 kg/m². This data differs from the literature, which suggests that gastroschisis is more commonly associated with malnourished pregnant women [18,19]. Studies even suggest an association between maternal obesity and a decreased risk of gastroschisis, which was not found in our study [20,21].
With respect to the association between obstetric characteristics and maternal diseases and neonatal death with gastroschisis, only gestational age at the beginning of prenatal care was statistically significant. Apparently, those who started prenatal care earlier had worse outcomes. This finding is contradictory to prenatal care guidelines, which recommend early initiation of prenatal care to improve postnatal outcomes [22]. This finding is also noteworthy because 50% of deaths occurred in neonates with simple gastroschisis.
Gestational age at diagnosis of gastroschisis was 21 weeks on average, four weeks shorter than in the study carried out in northern Brazil [22], highlighting the fact that only one case in our study had postnatal diagnosis. Studies show that lack of prenatal diagnosis is associated with a high mortality rate of gastroschisis in developing countries [13]. In Europe, between 2017 and 2021, more than 50% of gastroschisis cases were diagnosed < 14 weeks of gestational age and 35.4% between 14 and 23 weeks of gestation [12], probably because these countries invest in and recommend the performance of ultrasound for early diagnosis of congenital anomalies, and many of them even allow termination of pregnancy [23].
Regarding delivery characteristics, 98% of deliveries were by cesarean section, and the only newborn delivered vaginally had no prenatal diagnosis. The median gestational age was 36 weeks, with no differences in sex distribution, and the majority of newborns weighed > 2,000 grams. A Swedish study on the outcome and management of newborns with gastroschisis born between 1999 and 2020 after using a protocol showed a high frequency of survival, no deaths after 2005, favorable outcomes in terms of length of stay in the NICU, delivery by cesarean section in 92.1% of cases and a median of 36 weeks of gestational age at delivery [24].
The main clinical complications of gastroschisis identified in this study in the postnatal period were neonatal infection and sepsis, blood transfusion and hydroelectrolytic disorders. These complications are similar to those observed in the literature [22,25]. In a Brazilian study, 90.2% of 168 newborns with gastroschisis had postoperative infection and 41.3% had sepsis, with all infected newborns dying [22]. In our study, 5/16 newborns (31%) died due to infection, without statistical significance. Metabolic acidosis stood out as the main complication associated with neonatal death, affecting 6/16 newborns (38%). Metabolic acidosis was also the most common complication described in a study from Mexico, but it affected 32/42 newborns studied, accounting for 76% of cases, and led to death in 8/32 newborns (26%) [26]. The study suggests that the greater the amount of externalized intestine, the greater the risk of metabolic acidosis due to the production of a fetal inflammatory response due to exposure of the loops to amniotic fluid and that these changes contribute to fetal oxygen consumption [27].
During the study period, of the 46 newborns diagnosed with gastroschisis, all were admitted to the NICU with a mean length of stay of 39 days. Prolonged length of stay in the NICU is a relevant finding and is consistent with the literature [28,29]. A two-week shorter length of stay in the NICU was reported in a Swedish study that associated a reduction with the implementation of an institutional protocol [24].
Of the 46 cases of gastroschisis, 33 were classified as simple and 11 as complex, of which two were unclassified. Characterization regarding defect type was carried out in the postnatal period by describing the presence or absence of atresia, necrosis, perforation and volvulus [30]. We observed that, of the 11 cases of complex gastroschisis, 6 died, with a total of 55% of newborns. This finding is consistent with literature data showing higher morbidity and mortality in cases of complex gastroschisis [29].
Conclusion
In summary, we presented the epidemiological profile of pregnant women and the perinatal outcomes of newborns with gastroschisis at a tertiary care center in northeastern Brazil. We observed high rates of surgery with primary closure, blood transfusion and neonatal infection. Furthermore, we identified prolonged use of parenteral nutrition, long stay in the NICU, and prolonged use of antibiotic therapy.
Zdroje
1. Khan FA, Hashmi A. Insights into embryology and development of omphalocele. Semin Pediatr Surg 2019; 28 (2): 80–83. doi: 10.1053/j.sempedsurg.2019.04.003.
2. Suver D, Lee SL, Shekherdimian S et al. Left-sided gastroschisis: higher incidence of extraintestinal congenital anomalies. Am J Surg 2008; 195 (5): 663–666. doi: 10.1016/j.amjsurg.2007.12.042.
3. O’Connell RV, Dotters-Katz SK, Kuller JA et al. Gastroschisis: a review of management and outcomes. Obstet Gynecol Surv 2016; 71 (9): 537–544. doi: 10.1097/OGX.0000000000000344.
4. Bhat V, Moront M, Bhandari V. Gastroschisis: a state-of-the-art review. Children (Basel) 2020; 7 (12): 302. doi: 10.3390/children7120302.
5. Jones AM, Isenburg J, Salemi JL et al. Increasing prevalence of gastroschisis – 14 states, 1995–2012. Morb Mortal Wkly Rep 2016; 65 (2): 23–26. doi: 10.15585/mmwr.mm6502a2.
6. St. Louis AM, Kim K, Browne ML et al. Prevalence trends of selected major birth defects: a multi-state population-based retrospective study, United States, 1999 to 2007. Birth Defects Res 2017; 109 (18): 1442–1450. doi: 10.1002/bdr2.1113.
7. Egger PA, de Souza MP, de Oliveira Riedo C et al. Gastroschisis annual incidence, mortality, and trends in extreme Southern Brazil. J Pediatr (Rio J) 2023; 98 (1): 69–75. doi: 10.1016/j.jped. 2021.04.007.
8. Perrone EE, Olson J, Golden JM et al. Closing gastroschisis: the good, the bad, and the not so ugly. J Pediatr Surg 2019; 54 (1): 60–64. doi: 10.1016/j.jpedsurg.2018.10.033.
9. Barreiros CF, Gomes MA, Gomes Júnior SC. Mortality from gastroschisis in the state of Rio de Janeiro: a 10-year series. Rev Saude Publica 2020; 54 : 63. doi: 10.11606/s1518-8787. 2020054001757.
10. Muniz VM, Netto AL, Salaroli LB et al. Gastroschisis in Brazil within a global context. J Hum Growth Dev 2022; 32 (1): 83–91. doi: 10.36311/jhgd.v32.11796.
11. Marques AT, Estevão-Costa J, Soares H et al. Short and medium-term outcomes of omphalocele and gastroschisis: a survey from a tertiary center. Rev Bras Ginecol Obstet 2022; 44 (1): 10–18. doi: 10.1055/s-0041-1736299.
12. European Commission. Prevalence charts and tables. European Platform on Rare Disease Registration. 2024 [online]. Available from: https: //eu-rd-platform.jrc.ec.europa.eu/eurocat/eurocat-data/prevalence_en.
13. Fatona O, Opashola K, Faleye A et al. Gastroschisis in Sub-Saharan Africa: a scoping review of the prevalence, management practices, and associated outcomes. Pediatr Surg Int 2023; 39 (1): 246. doi: 10.1007/s00383-023-05531-w.
14. Regadas CT, Escosteguy CC, Fonseca SC et al. Trends in prevalence of gastroschisis in Brazil from 2007 to 2020: a national population-based cross-sectional study. Birth Defects Res 2023; 115 (6): 633–646. doi: 10.1002/bdr2.2156.
15. Brebner A, Czuzoj-Shulman N, Abenhaim HA. Prevalence and predictors of mortality in gastroschisis: a population-based study of 4803 cases in the USA. J Matern Fetal Neonatal Med 2020; 33 (10): 1725–1731. doi: 10.1080/14767058.2018.1529163.
16. Michikawa T, Yamazaki S, Suda E et al. Does overweight before pregnancy reduce the occurrence of gastroschisis? the Japan Environment and Children’s Study. BMC Res Notes 2020; 13 (1): 47. doi: 10.1186/s13104-020-4915-7.
17. Morris JK, Wellesley D, Limb E et al. Prevalence of vascular disruption anomalies and association with young maternal age: a EUROCAT study to compare the United Kingdom with other European countries. Birth Defects Res 2022; 114 (20): 1417–1426. doi: 10.1002/bdr2.2122.
18. Siega‐Riz AM, Herring AH, Olshan AF et al. The joint effects of maternal prepregnancy body mass index and age on the risk of gastroschisis. Paediatr Perinat Epidemiol 2009; 23 (1): 51–57. doi: 10.1111/j.1365-3016.2008.00990.x.
19. Feldkamp ML, Carmichael SL, Shaw GM et al. Maternal nutrition and gastroschisis: findings from the National Birth Defects Prevention Study. Am J Obstet Gynecol 2011; 204 (5): 404.e1–404.e10. doi: 10.1016/j.ajog.2010.12.053.
20. Khodr ZG, Lupo PJ, Canfield MA et al. Hispanic ethnicity and acculturation, maternal age and the risk of gastroschisis in the national birth defects prevention study. Birth Defects Res Part A Clin Mol Teratol 2013; 97 (8): 538–545. doi: 10.1002/bdra.23140.
21. Jenkins MM, Reefhuis J, Gallagher ML et al. Maternal smoking, xenobiotic metabolizing enzyme gene variants, and gastroschisis risk. Am J Med Genet A 2014; 164 (6): 1454–1463. doi: 10.1002/ajmg.a.36478.
22. Bilibio JP, Beltrão AM, Vargens AC et al. Gastroschisis during gestation: prognostic factors of neonatal mortality from prenatal care to postsurgery. Eur J Obstet Gynecol Reprod Biol 2019; 237 : 79–84. doi: 10.1016/j.ejogrb.2019.04.015.
23. Baumann S, Darquy S, Miry C et al. Termination of pregnancy for foetal indication in the French context analysis of decision-making in a Multidisciplinary Centre For Prenatal Diagnosis. J Gynecol Obstet Hum Reprod 2021; 50 (8): 102067. doi: 10.1016/j.jogoh.2021.102067.
24. Räsänen L, Lilja HE. Outcome and management in neonates with gastroschisis in the third millennium – a single-centre observational study. Eur J Pediatr 2022; 181 (6): 2291–2298. doi: 10.1007/s00431-022-04416-9.
25. Dekonenko C, Fraser JD, Deans KJ et al. Outcomes in gastroschisis: expectations in the post--natal period for simple vs complex gastroschisis. J Perinatol 2021; 41 (7): 1755–1759.
26. Méndez-Martínez S, García-Carrasco M, Mendoza-Pinto C et al. Surgical complications of simple and complex gastroschisis in newborn. Eur J Gen Med 2016; 13 (2): 88–93. doi: 10.15197/ejgm.1495.
27. Moore P, Vogt S, Guerra FA. Acidosis predictive factors in fetal gastroschisis. Ultrasound Obstet Gynecol 2017; 50 (S1): 310. doi: 10.1002/uog.18503.
28. Youssef F, Laberge JM, Puligandla P et al. Determinants of outcomes in patients with simple gastroschisis. J Pediatr Surg 2017; 52 (5): 710–714. doi: 10.1016/j.jpedsurg.2017.01.019.
29. Jaczyńska R, Mydlak D, Mikulska B et al. Perinatal outcomes of neonates with complex and simple gastroschisis after planned peterm delivery – a single-centre retrospective cohort study. Diagnostics (Basel) 2023; 13 (13): 2225. doi: 10.3390/diagnostics13132225.
30. Molik KA, Gingalewski CA, West KW et al. Gastroschisis: a plea for risk categorization. J Pediatr Surg 2001; 36 (1): 51–55. doi: 10.1053/ jpsu. 2001.20004.
ORCID of authors
C. M. G. C. Escoto Esteche 0000-0001-6958-3185
E. Araujo Júnior 0000-0002-6145-2532
B. C. Escoto Esteche 0009-0004-3899-321X
L. C. Rolo 0000-0002-8739-4115
Submitted/Doručeno: 14. 7. 2025
Accepted/Přijato: 6. 10. 2025
Prof. Edward Araujo Júnior, MD, PhD
Rua Belchior de Azevedo
156 apto. 111 Torre Vitoria
Vila Leopoldina
CEP 05089-030
São Paulo-SP, Brazil
araujojred@terra.com.br
Štítky
Dětská gynekologie Gynekologie a porodnictví Reprodukční medicínaČlánek vyšel v časopise
Česká gynekologie

2026 Číslo 1
Nejčtenější v tomto čísle
- Pelvic floor muscles High-Intensity Tesla Stimulation
- Cervical cancer screening in the European context – from cytology to primary HPV testing
- Molar ectopic pregnancy in a cesarean scar treated with methotrexate – a case report and review of the literature
- Cytological versus histological results in ASCUS cervical dysplasia – a retrospective study