
Molar ectopic pregnancy in a cesarean scar treated with methotrexate – a case report and review of the literature
Authors:
E. Yücel 1
![]() ; İbrahim Kale 1
; İbrahim Kale 1
![]() ; O. Şanlı 1
; O. Şanlı 1
![]() ; A. N. İhvan 2
; A. N. İhvan 2
![]()
Authors place of work:
Department of Obstetrics and Gynecology, Umraniye Training and Research Hospital, Istanbul, Turkey
1; Department of Pathology, Umraniye Training and Research Hospital, Istanbul, Turkey
2
Published in the journal:
Ceska Gynekol 2026; 91(1): 56-60
Category:
Kazuistika
doi:
https://doi.org/10.48095/cccg202656
Summary
Objective: To present a rare case of partial molar pregnancy implanted in a previous cesarean section scar and summarize the literature. Case report: A 33-year-old woman (gravida 5, two prior cesarean deliveries, two spontaneous abortions) presented with vaginal spotting and lower abdominal pain at 6 weeks of gestation. Transvaginal ultrasonography revealed a 28 × 19 mm gestational sac at the cesarean scar site, containing a 4mm fetus with positive cardiac activity. Vacuum curettage was performed under ultrasonographic guidance. Ten days postprocedure, rising serum beta-hCG levels and a persistent cystic mass on ultrasound raised suspicion for molar pregnancy. A single systemic dose of methotrexate was administered. Histopathology confirmed a partial molar pregnancy. The patient’s serum beta-hCG levels normalized within 8 weeks. Conclusion: Partial molar pregnancy in a cesarean section scar is an extremely rare condition that may present with vaginal bleeding and pelvic pain. Early recognition through ultrasonography and laboratory evaluation, combined with timely intervention including curettage and methotrexate therapy, can lead to complete resolution. Clinicians should consider this diagnosis in patients with previous cesarean sections to ensure optimal outcomes.
Keywords:
jizva po císařském řezu – molární těhotenství – částečný hydatidiformní mol – methotrexát – vakuová kyretáž
Backgroud
Cesarean scar pregnancy (CSP) is a rare form of ectopic pregnancy in which the gestational sac implants into the myometrium at the site of a previous cesarean section scar. CSP was first described in the literature by Larsen and Solomon in 1978 [1]. As cesarean section rates have increased over the years, the incidence of CSP has also risen, currently estimated to occur in approximately 1 in 2,216 pregnancies [2].
Gestational trophoblastic disease encompasses a broad spectrum of benign and malignant disorders arising from the trophoblastic cells of the placenta. While partial hydatidiform mole and complete hydatidiform mole represent the benign forms, the malignant variants include invasive mole, gestational choriocarcinoma, placental site trophoblastic tumor, and epithelioid trophoblastic tumor [3]. The incidence of hydatidiform mole ranges from 0.04–0.9%, depending on the population’s ethnic background [4–6]. The presence of a hydatidiform mole within a cesarean scar, representing the coexistence of two rare conditions, constitutes an extremely uncommon clinical entity.
Here, we report a rare case of molar pregnancy occurring at the site of a previous cesarean section scar.
Own observation
A 33-year-old woman presented with vaginal spotting and lower abdominal pain following approximately 2 months of amenorrhea. Based on her last menstrual period, she was estimated to be 6 weeks and 4 days pregnant. This was her 5th pregnancy; her obstetric history included two prior cesarean deliveries and two spontaneous abortions. On sterile speculum examination, the vagina appeared normal, the cervix had a nulliparous appearance, and there was spotting-type bleeding. Transvaginal ultrasonography revealed an anteverted uterus with an endometrial thickness of 11 mm at the fundal level. A gestational sac measuring 28 × 19 mm was observed below the previous cesarean scar, containing a fetus with a crown-rump length (CRL) of 4 mm and positive fetal cardiac activity, corresponding to a gestational age of 6 weeks and 1 day. The cervix was closed, and the cervical length measured 31 mm (Fig. 1). Both ovaries appeared normal on ultrasound.

As fetal cardiac activity was observed, a serum beta-hCG test was not requested. Based on the patient’s clinical and ultrasonographic findings, a diagnosis of cesarean scar ectopic pregnancy was established. Following detailed counseling and the acquisition of written informed consent from the patient and her husband, dilatation and curettage were performed under general anesthesia with suprapubic ultrasonographic guidance for CSP termination. Following curettage, a Foley catheter was inserted into the uterine cavity to prevent potential hemorrhage from the cesarean scar, and the balloon was inflated with 30 mL at the scar level. The catheter was removed appropriately one day after the procedure. The patient, who experienced no postoperative bleeding, was discharged in stable condition.
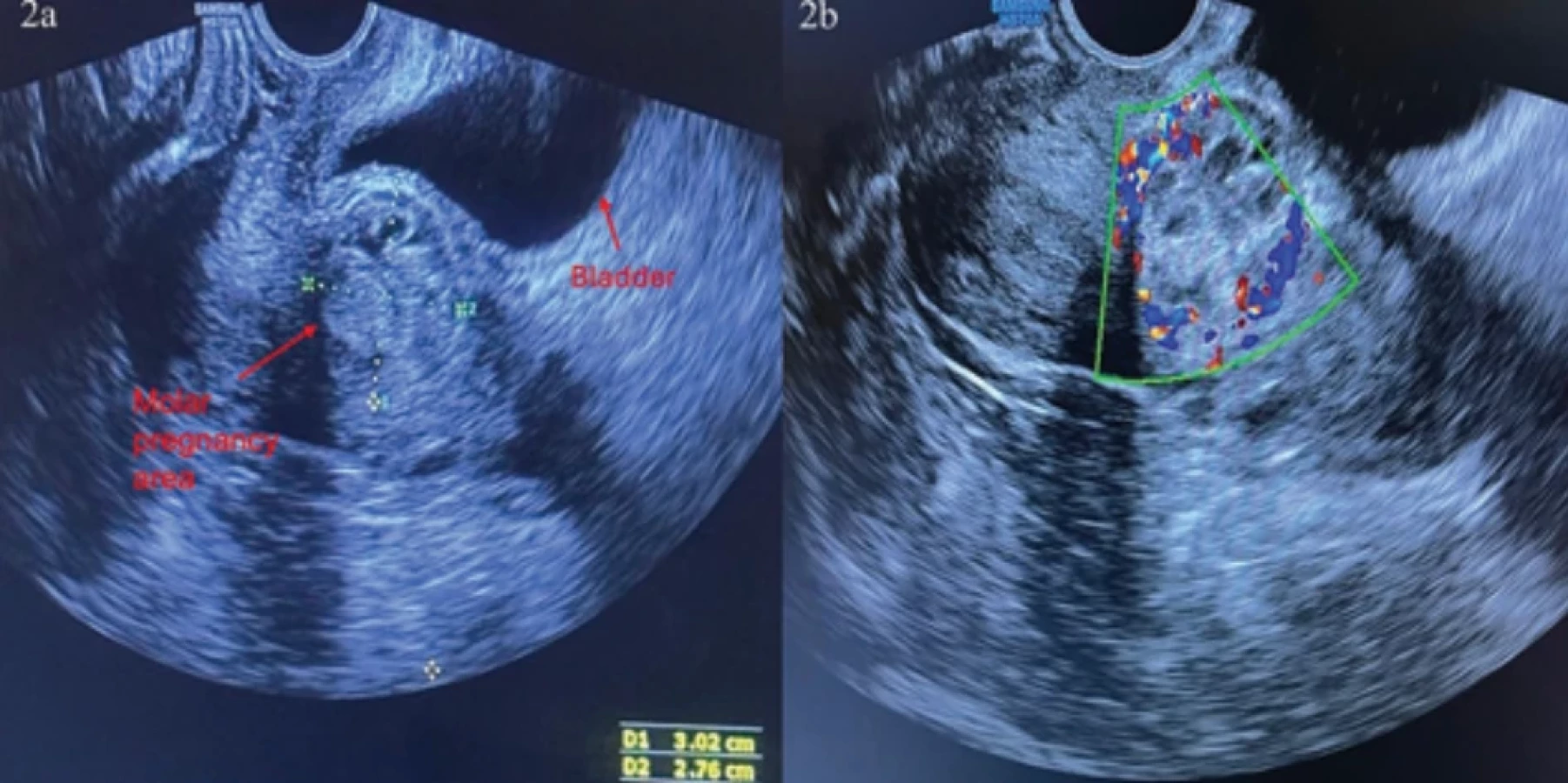
The patient’s serum beta-hCG level measured 6 days after the procedure was 10,746 mIU/mL, and ten days later, it had risen to 11,469 mIU/mL. A transvaginal ultrasound performed ten days post-procedure revealed a 27 × 30 mm heterogeneous cystic mass extending outward from the cesarean scar site, with detectable blood flow on Doppler imaging (Fig. 2). The combination of rising serum beta-hCG levels and ultrasound findings raised suspicion for a molar pregnancy. The patient and her husband were informed of the clinical findings. Laboratory investigations and a chest X-ray were performed, all of which were within normal limits. The hospital’s pathology department was contacted to expedite the pathological evaluation. Meanwhile, the patient was administered a single dose of methotrexate (50 mg/m²). Seventeen days after the procedure, the pathology report confirmed the diagnosis of a partial molar pregnancy (Fig. 3). During follow-up, the patient’s serum beta-hCG level became negative approximately 8 weeks after the procedure. The heterogeneous cystic appearance previously observed at the cesarean scar site on ultrasound resolved by approximately 8 weeks.

Discussion
CSP and GTD are rare conditions; our case of cesarean scar molar pregnancy, which combines these two pathologies, is therefore extremely rare. In cases where timely diagnosis is not established and the appropriate treatment procedure is not applied, the risk of hemorrhage and uterine rupture is high. Despite these risks, data regarding the optimal management of cesarean scar molar pregnancy remain limited.
We conducted a literature review to identify cases similar to this pathology, which has a low incidence. To the best of our knowledge, only 13 cases have been reported in the literature (Tab. 1) [7–19]. The first documented case was reported in 2006 by Wu et al. In the case reported by Wu et al., molar pregnancy was suspected based on ultrasound findings and b-hCG levels, and suction curettage was performed. A second vacuum aspiration was performed for the patient with persistent vaginal bleeding [7]. Since this case, various cases of cesarean scar molar pregnancy have been described, in which different diagnostic methods and treatment modalities were applied. The most common presenting symptom is vaginal bleeding, which is usually followed by pelvic pain. Of the 13 cases reported in the literature, 10 presented to the hospital with vaginal bleeding, similar to our case. The other symptoms include inguinal pain and unexplained pregnancy-related signs. Three patients were reported to be asymptomatic.
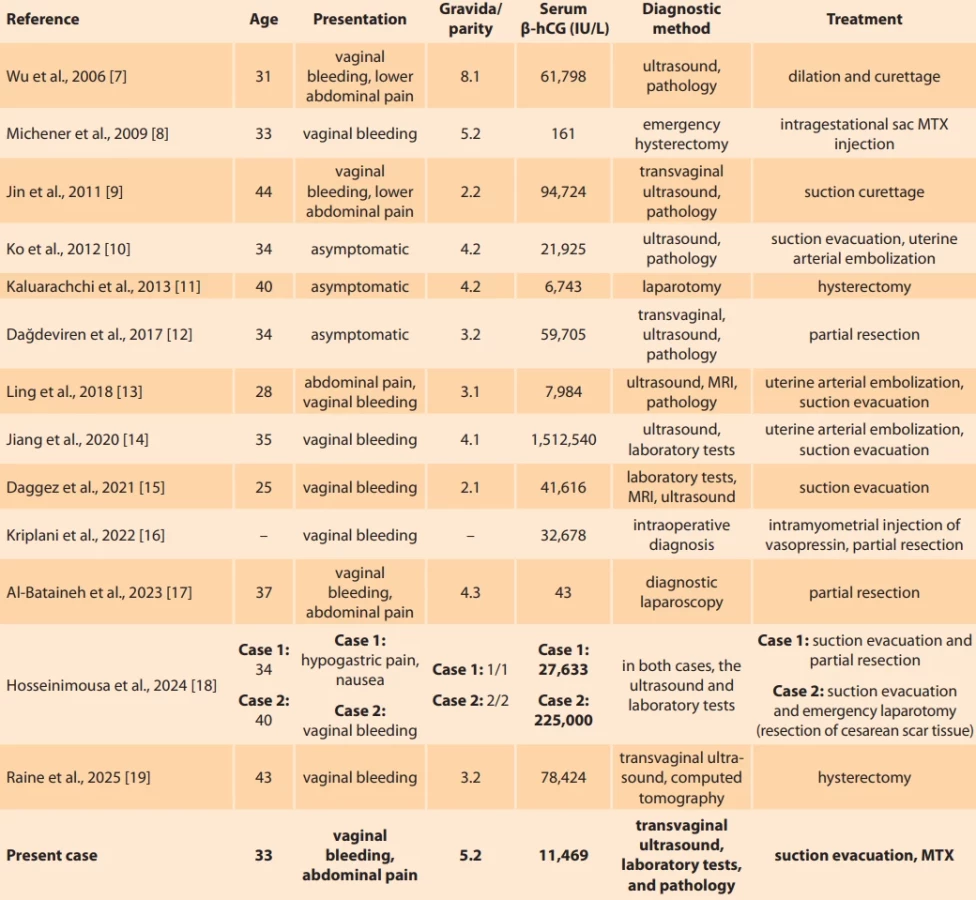
In case reports, diagnostic methods show that ultrasound is the most frequently used modality. Laboratory results follow this. Other diagnostic procedures include histopathological examination, magnetic resonance imaging (MRI), computed tomography (CT), and, in some cases, surgical exploration. In our case, the diagnosis was established based on laboratory tests, ultrasound, and pathological examination. Curettage was performed in 8 of the 13 patients, uterine artery embolization in 3, partial resection in 4, and hysterectomy in 2. Michener and Dickinson applied a different treatment procedure; they injected methotrexate into the intragestational sac and subsequently administered systemic methotrexate to induce a plateau in b-hCG levels. During follow-up, an emergency hysterectomy was performed ten months later due to the occurrence of bleeding [8].
In our case, the patient initially underwent vacuum curettage. Ten days later, molar pregnancy was suspected, and a single systemic dose of methotrexate was administered, resulting in complete recovery. Histopathological examination confirmed the diagnosis of partial molar pregnancy.
Conclusion
This case report presents the clinicopathological features and successful management of an ectopic molar pregnancy in a cesarean scar that resulted in cure. Clinicians should maintain a high index of suspicion for this rare pathology. This case report, supported by a literature review, summarizes the diagnostic and therapeutic approaches to cesarean scar molar pregnancy, emphasizing the necessity of patient-specific, multidisciplinary treatment plans.
Zdroje
1. Larsen JV, Solomon MH. Pregnancy in a uterine scar sacculus – an unusual cause of postabortal haemorrhage. A case report. S Afr Med J 1978; 53 (4): 142–143.
2. Seow KM, Huang LW, Lin YH et al. Cesarean scar pregnancy: issues in management. Ultrasound Obstet Gynecol 2004; 23 (3): 247–253. doi: 10.1002/uog.974.
3. Seckl MJ, Sebire NJ, Fisher RA et al. Gestational trophoblastic disease: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2013; 24 (Suppl 6): vi39–vi50. doi: 10.1093/annonc/mdt345.
4. Altalib A, Al Qahtani N, Alosaimi SS et al. Changing trends in the clinical presentation and incidence of molar pregnancy in Saudi Arabia: a 30-year retrospective analysis. Cureus 2023; 15 (12): e50936. doi: 10.7759/cureus.50936.
5. González Mariño MA. A cross-sectional analysis of the incidence of hydatidiform mole in Colombia. Obstet Gynecol Int 2025; 2025 : 8899358. doi: 10.1155/ogi/8899358.
6. Kale İ. Evaluation of gestational trophoblastic diseases; 10 years’ experience in tertiary obstetric care center. Zeynep Kamil Med J 2021; 52 (4): 170–176. doi: 10.14744/zkmj.2021. 04557.
7. Wu CF, Hsu CY, Chen CP. Ectopic molar pregnancy in a cesarean scar. Taiwan J Obstet Gynecol 2006; 45 (4): 343–345. doi: 10.1016/S10 28-4559 (09) 60257-6.
8. Michener C, Dickinson JE. Caesarean scar ectopic pregnancy: a single centre case series. Aust N Z J Obstet Gynaecol 2009; 49 (5): 451–455. doi: 10.1111/j.1479-828X.2009.01067.x.
9. Jin FS, Ding DC, Wu GJ et al. Molar pregnancy in a cesarean section scar of uterus. J Med Sci 2011; 31 (4): 173–176.
10. Ko JK, Wan HL, Ngu SF et al. Cesarean scar molar pregnancy. Obstet Gynecol 2012; 119 (2 Pt 2): 449–451. doi: 10.1097/AOG.0b013e3182322f31.
11. Kaluarachchi CI, Tissera AJ, Karunarathna SG. Caesarean scar site complete molar pregnancy. Sri Lanka J Obstet Gynaecol 2013; 35 : 62–64. doi: 10.4038/sljog.v35i2.6162.
12. Dağdeviren EG, Dur R, Fadıloğlu E et al. Molar pregnancy in cesarean section scar: a case report. Turk J Obstet Gynecol 2017; 14 (4): 249–251. doi: 10.4274/tjod.26878.
13. Ling C, Zhao J, Qi X. Partial molar pregnancy in the cesarean scar: a case report and literature review. Medicine (Baltimore) 2018; 97 (26): e11312. doi: 10.1097/MD.00000000000 11312.
14. Jiang HR, Shi WW, Liang X et al. Hydatidiform mole in a scar on the uterus: a case report. World J Clin Cases 2020; 8 (8): 1547–1553. doi: 10.12998/wjcc.v8.i8.1547.
15. Daggez M, Dolanbay M. Molar pregnancy in cesarean section scar: a case report and literature review. Z Geburtshilfe Neonatol 2021; 225 (3): 275–278. doi: 10.1055/a-1237-4506.
16. Kriplani I, Srivastava V, Bhardwaj K et al. Laparoscopic management of partial molar caesarean scar ectopic pregnancy. J Minim Invasive Gynecol 2022; 29 (11): 1221–1223. doi: 10.1016/j.jmig.2022.08.008.
17. Al-Bataineh R, Rawashdeh S, Lataifeh LN et al. Cesarean scar ectopic partial molar pregnancy: a case report and a review of literature. Case Rep Womens Health 2023; 39: e00555. doi: 10.1016/j.crwh.2023.e00555.
18. Hosseinimousa S, Navaei S, Talebian M. Molar cesarean scar ectopic pregnancy: report of 2 cases with review of literature. Int J Reprod Biomed 2024; 22 (2): 161–168. doi: 10.18502/ijrm.v22i2.15714.
19. Raine SR, Schulte V, Floyd J et al. Critical diag - nosis and management of a case of a partial molar cesarean scar ectopic pregnancy. Cureus 2025; 17 (2): e79009. doi: 10.7759/cureus.79009.
ORCID of authors
E. Yücel 0000-0002-5941-1926
İ. Kale 0000-0001-7802-7199
O. Şanlı 0009-0001-4737-0872
A. N. İhvan 0009-0009-3843-9688
Submitted/Doručeno: 1. 9. 2025
Accepted/Přijato: 5. 10. 2025
Assoc. Prof. İbrahim Kale, MD
Department of Obstetrics and Gynecology
Umraniye Training and Research Hospital
Elmalıkent, Adem Yavuz Cd.
34764 Ümraniye/İstanbul
Turkey
dribakale@hotmail.com
Štítky
Dětská gynekologie Gynekologie a porodnictví Reprodukční medicínaČlánek vyšel v časopise
Česká gynekologie

2026 Číslo 1
Nejčtenější v tomto čísle
- Pelvic floor muscles High-Intensity Tesla Stimulation
- Cervical cancer screening in the European context – from cytology to primary HPV testing
- Molar ectopic pregnancy in a cesarean scar treated with methotrexate – a case report and review of the literature
- Cytological versus histological results in ASCUS cervical dysplasia – a retrospective study