
Prenatal sonographic features and outcomes of radial ray defects – a 14 case series with a literature review
Authors:
G. Ünver 1
![]() ; S. Serin 1
; S. Serin 1
![]() ; M. Tosun 1
; M. Tosun 1
![]() ; H. Çelik 1
; H. Çelik 1
![]() ; M. Önal 1
; M. Önal 1
![]() ; Ü. Abur 2
; Ü. Abur 2
![]() ; E. Altundağ 2
; E. Altundağ 2
![]()
Authors place of work:
Department of Obstetrics and Gynecology, Perinatology Unit, Faculty of Medicine, Ondokuz Mayis University, Samsun, Turkey
1; Department of Medical Genetics, Faculty of Medicine, Ondokuz Mayis University, Samsun, Turkey
2
Published in the journal:
Ceska Gynekol 2026; 91(1): 35-40
Category:
Původní práce
doi:
https://doi.org/10.48095/cccg202635
Summary
Objective: In this study, we aimed to present the demographic, ultrasonographic, genetic, obstetric, and postpartum results of 14 patients diagnosed with radial ray defects. Materials and methods: Fourteen patients diagnosed with radial ray defects. Non-development or hypoplasia of any preaxial part of the upper extremity on ultrasonography was considered a radial ray defect. Maternal age, gestational week at diagnosis, laterality of the radial ray defect, genetic results, presence of comorbid anomalies, termination status, and postpartum prognosis were obtained. Results: The range of maternal age at the time of diagnosis was 17–38 years and the gestational age ranged between 14–26 weeks. Four of the radial ray defects were bilateral, and ten were unilateral. Trisomy 18 was identified in two cases. Eight cases accepted the termination procedure. Three cases rejected termination and had spontaneous intrauterine death during pregnancy follow-up. One case was diagnosed with VACTERL association and died postpartum on the 13th day. One case was monitored due to Fanconi aplastic anemia and one case had amniotic band syndrome in etiology and lives with a prosthetic arm. Conclusion: The frequency of a radial ray defect accompanied by syndromic and congenital anomalies was high, and visualization of the radial bone or other preaxial bone structures on the 1st trimester fetal ultrasonography will ensure the diagnosis of a radial ray defect in early gestational weeks. In the case of a radial ray defect diagnosis, systemic organ screening should be performed with detailed ultrasonography and the necessary invasive procedure for karyotype examination should be advised to all families.
Keywords:
Antenatal care – prenatal diagnosis – early screening – 1st trimester screening – radial ray defect – radial ray malformation
Introduction
Radial ray defects (RRD) are characterized by developmental defects that involve the preaxial parts of the upper extremity (radius, scaphoid, and trapezium bones, metacarpal, and phalangeal structures of the thumb). Any of these bones may have hypoplasia or aplasia, or hypoplasia/aplasia of more than one bone may accompany each other [1].
The incidence of upper extremity defects in the fetus is 5.56 per 10,000 births [2]. The incidence of radial ray defect, which is the most common congenital anomaly of the upper extremity, is 1.83 per 10,000 in fetal life [2].
The radial ray defect is isolated in approximately 30% of cases, whereas it may be accompanied by additional anomalies, chromosomal disorders, and syndromes in 70% of cases [3]. In recent studies, the frequency of accompanying anomalies has been reported to be higher in fetuses with radial ray defects, and only 13% of cases have been identified as isolated radial ray defects [1].
The rate of chromosomal disorders accompanying radial ray defects is approximately 28% and the most common chromosomal disorder is trisomy 18 [1]. The most common comorbid syndromes include Fanconi anemia, Thrombocytopenia-Bilateral Absent Radius syndrome (TAR), Holt-Oram syndrome, and VACTERL association [3,4].
In this study, we aimed to emphasize the relationship between radial ray defects and underlying syndromes, their coexistence with genetic diseases, accompanying anatomical anomalies, and their etiologies.
Material and methods
Study design
In this study, 14 patients who were diagnosed with radial ray defects between 2012 and 2025 at the Perinatology Clinic of Samsun Ondokuz Mayıs University were included. Ethics committee approval was obtained from Ondokuz Mayıs University Faculty of Medicine. Ethics Committee with the decision numbered B.30.2.ODM.0.20.08/ 513-678.
Patients selection
Non-development or hypoplasia of any preaxial part of the upper extremity (radius, scaphoid, trapezoid bone, and thumb) on ultrasonography was considered a radial ray defect. Prenatal exposure to thalidomide, valproic acid, or any known teratogenic agent was questioned in the anamnesis. All patients were screened for the etiology of diabetic embryopathy through a 75 grams oral glucose tolerance test.
Data and measurements
The maternal age of the cases, gestational week at diagnosis, laterality of the radial ray defect, genetic results, presence of comorbid anomalies, termination status, and postnatal prognosis were obtained from the hospital records. Patients who could not be followed up in our hospital were reached by phone, and information about their children’s prognosis was obtained.
All pregnant women in whom radial ray defects were detected on ultrasonography were recommended karyotyping for prenatal diagnosis and genetic counseling was provided. Pregnant women who accepted karyotype analysis underwent amniocentesis and cordocentesis. All cases were evaluated by a council consisting of perinatology, pediatrics, and medical genetics physicians, and a termination option was offered.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation.
Results
The range of maternal age at the time of diagnosis was 17–38 years, and the gestational age ranged between 14–26 weeks. In the evaluation, four of the radial ray defects were bilateral, and ten were unilateral (Tab. 1). Teratogen exposure and diabetes mellitus were not identified in any case.

termination, w – week
Invasive procedures were recommended for all cases for genetic examination; amniocentesis was performed in eight cases, and cordocentesis was performed in one case. Seven patients had normal karyotype results, and two cases had trisomy 18. Five cases rejected the invasive procedure.
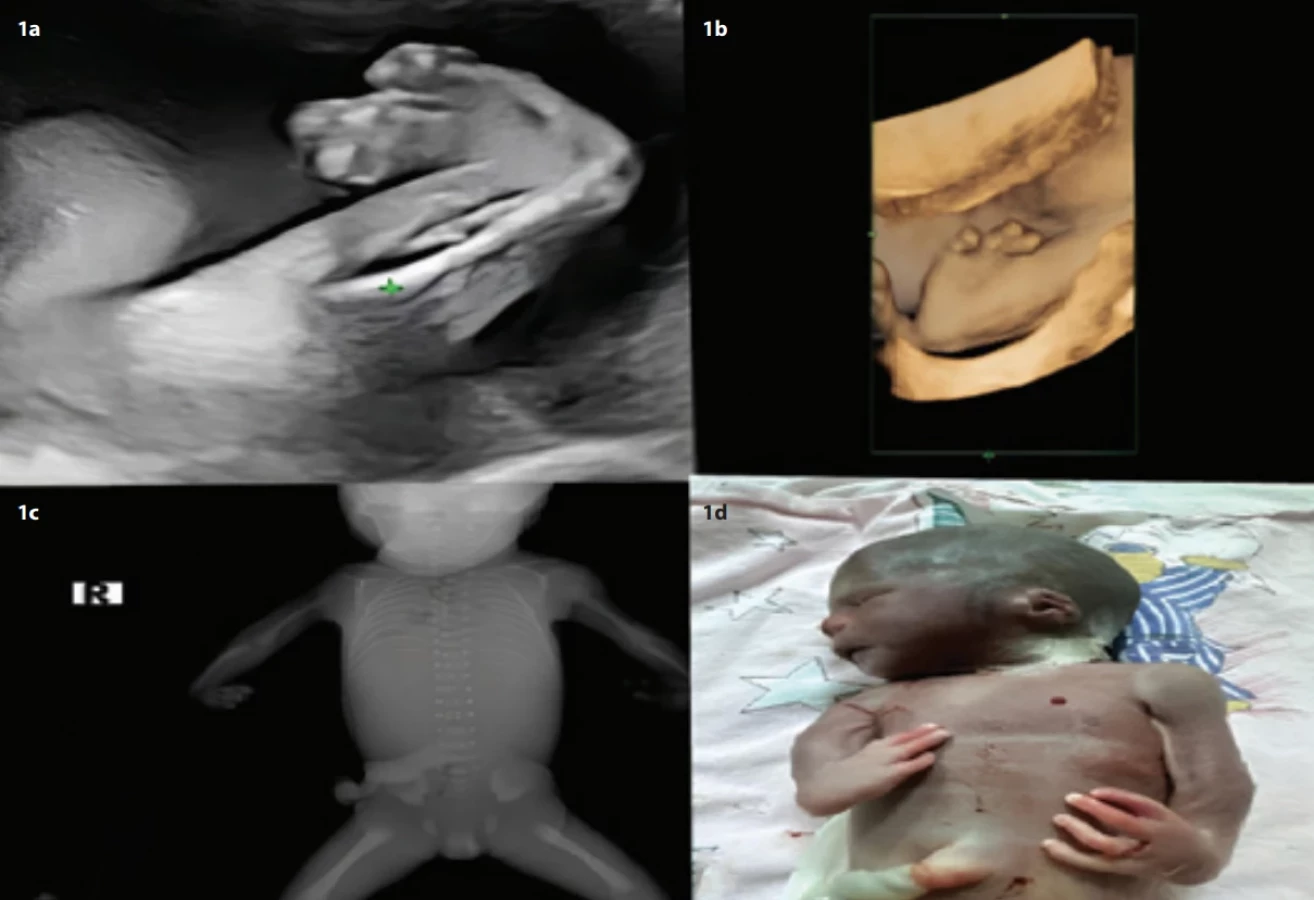
Cases 1, 2, and 3 had isolated unilateral radius aplasia. All three cases had normal karyotype results, and the pregnancies were terminated upon patient request and council’s decision (Fig. 1c shows radial deviation postmortem X-ray).
Cases 4 and 5 had ulnar hypoplasia along with unilateral radial ray defect. The karyotype results of both cases were normal. The pregnancy was terminated in case four whereas case five was 3-years-old and developed radial ray defect due to amniotic band syndrome and was living with a prosthetic arm.
Among the two cases who were diagnosed with trisomy 18 as a result of amniocentesis, case 6 had aplasia of the radius as unilateral radial ray defect, aplasia of the first and second fingers of the left hand, and alobar holoprosencephaly and atrioventricular septal defect. Case 7 had unilateral radius aplasia, choroid plexus cyst, ventricular septal defect, and omphalocele. Pregnancy was terminated in both cases as a result of the council’s decision.
In cases 9 and 8, neural tube defects were detected in addition to aplasia of the radius. Case eight was bilateral while case nine was unilateral. In case eight, the family rejected karyotype analysis and pregnancy termination. At gestational week 28, intrauterine fetal death occurred. In case nine, which was unilateral, the family rejected the karyotype analysis, and the pregnancy was terminated.
Case 10 had bilateral radius, first metacarpal, and first phalanx aplasia accompanied by ventriculomegaly, microcephaly, microphthalmia, tracheoesophageal fistula, and atrial septal defect. The family rejected the karyotype analysis and wanted to continue the pregnancy. After delivery, the baby was operated on for tracheoesophageal fistula and followed up with the diagnosis of VACTERL association until the age of 2 years. The case, who was currently 8-years-old, had negative diepoxybutane and mitomycin C chromosomal breakage tests and was followed up by the pediatric hematology clinic for the diagnosis of Fanconi anemia due to the development of pancytopenia clinic and hypocellular appearance in bone marrow biopsy.
Case 11 had brachycephaly, cleft palate, atrial septal defect, and horseshoe kidney along with bilateral radius aplasia. The baby of the family who rejected the karyotype analysis died in utero on the 13th day postpartum.
Case 12 had bilateral radius aplasia, right first and second fingers and left thumb aplasia as bilateral radial ray defects, accompanied by monoventricle, double outlet right ventricle, absence of stomach, single umbilical artery, low ear, and lymphocyst in the neck. Cordocentesis was performed to exclude the diagnosis of Thrombocytopenia-Bilateral Absent Radius syndrome (TAR), and microarray analysis of the fetus with normal platelet count was normal. The pregnancy was terminated upon family request (Fig. 1a, b, d shows case 12 fetal ultrasound and necropsy findings). Both cases were recognized as VACTERL associations.
In case 13, atrioventricular septal defect, choroid plexus cyst, and strawberry head were detected in addition to unilateral radius aplasia. The case was thought to possibly have trisomy 18, but the family rejected karyotyping, and no definitive diagnosis could be made. The fetus died in utero at the 36th gestational week.
In case 14, at 15 weeks of gestation, a spontaneous monochorionic monoamniotic twin pregnancy was diagnosed. The first fetus had a left-sided congenital diaphragmatic hernia, and the second fetus had exencephaly and right radial ray defect (Fig. 2a, b). Amniocentesis revealed a normal karyotype. Targeted gene panel analysis (including Fanconi anemia, Holt-Oram syndrome, and related disorders) yielded normal results. Pregnancy was terminated in this case as a result of the council’s decision.

Discussion
Differentiation and developmental problems during the formation of extremities, which starts on the 26th to 28th day after fertilization and is completed in 4 weeks, lead to extremity defects [5].
Radial ray defect is the most common congenital anomaly of the upper extremity. It should be suspected in the presence of persistent abnormal hand position and fixed flexion of the wrist.
Radius measurement is not part of routine fetal biometry. Shortening or absence of the radius bone on fetal sonography, abnormal angle between the forearm and palm, and abnormal deviation of the fingers, especially the thumb, are important in the diagnosis.
In a series of 138 cases of radial ray defects conducted by Niklas et al., 13% of the cases were isolated and 59% were bilateral. In the present study, approximately 23% of the cases were isolated and 30% were bilateral radial ray defects [1]. In the same study, the male/female ratio for radial ray defects was reported to be 1.4, whereas the male/female ratio was determined as 1.6 in our cases. As in the study of Black et al., male gender was a risk factor for radial ray defects in our patients [6].
The most common chromosomal abnormality in radial ray defect is trisomy 18 and in the study by Niklas et al., the rate of trisomy 18 was reported to be 23%. Among our 13 patients, trisomy 18 was confirmed in two of the eight patients who accepted the karyotype analysis. In one case, although the risk of trisomy 18 was estimated to be 1/50 in the triple screening test and ultrasonographic findings included strawberry head shape, atrioventricular septal defect, and choroid plexus cyst in favor of trisomy 18, the patient rejected the karyotype analysis. The fetus died in utero at the 38th gestational week. It was thought that this case might have trisomy 18 [1].
VACTERL association refers to vertebral anomalies (V), anal atresia (A), cardiac defects (C), tracheo-esophageal fistula (TE), renal malformation (R), and limb anomalies (L). VACTERL association is diagnosed when any three of these anomalies are present together. Cases with VACTERL association are classified into three groups according to extremity anomalies: VACTERL 1 diagnosis includes cases with normal extremities, VACTERL 2 with extremity anomalies other than radial ray defects of the upper extremities, and VACTERL 3 with radial ray defects of the upper extremities [7].
In the series of Niklas et al., 20% of the cases were associated with VACTERL association. Two of our 13 cases (case 11 and case 12) met at least three criteria for VACTERL association. Although two cases (case 8 and case 9) were found to have vertebral anomalies and radial ray defects, the third criterion for VACTERL association could not be documented because the families rejected the recommendation for autopsy after termination. According to some opinions, two criteria are sufficient for the diagnosis of VACTERL association [8].
Fanconi anemia is an autosomal recessive inherited DNA repair disorder characterized by physical abnormalities and increased susceptibility to malignancies. Thumb and radius hypoplasia are the most common extremity defects accompanying Fanconi anemia [9]. Although one of our cases was diagnosed with bilateral radial ray defect, ventriculomegaly, microphthalmia, tracheoesophageal fistula, and atrial septal defect, the family rejected the karyotype analysis. The case was followed up until the age of 2 years with the diagnosis of VACTERL association and was followed up with the diagnosis of Fanconi aplastic anemia due to the development of pancytopenia and hypocellularity in bone marrow biopsy.
Solomon and Alter-Rosenber extensively discussed the clinical overlap between the VACTERL-Hydrocephalus association and Fanconi anemia. In this study, it was suggested that patients with Fanconi aplastic anemia associated with VACTERL-ventriculomegaly could be immediately recognized by the “FA VATER signal”, which should lead to FA testing [9]. The antenatal diagnosis of bilateral radial ray defect (absence of radius and thumb) and ventriculomegaly was significant in terms of “FA VATER signal” for the case in our study.
The coexistence of exencephaly-anencephaly sequence (case 14) and radial ray defects suggests a severe disruption in early neural tube and limb field development, possibly linked to defective Wnt/b-catenin signaling pathways. This rare phenotypic combination may indicate an underlying syndromic etiology, such as Fanconi anemia or VACTERL association, where both CNS and limb malformations are reported [10]. Given the poor prognosis of this malformation complex, prenatal genetic testing (whole-exome-sequencing) is warranted to identify potential mutations which are implicated in both cranial and limb defects. This case highlights both the constraints of targeted gene panels and the necessity of exome sequencing in evaluating complex prenatal anomalies.
The type of radial ray defects does not affect the mode of delivery. Delivery in a tertiary health center with pediatric, genetic, and orthopedic surgical consultation should be considered in line with clinical findings. After delivery, the baby should be referred to a specialist for potential reconstructive surgery. Radial ray defects associated with other system anomalies or syndromes are treated according to the severity of findings.
Isolated findings are usually sporadic, and the risk of recurrence is low. The recurrence of syndromic cases depends on the underlying cause.
Termination of pregnancy should be discussed as an option for all patients with radial ray defects. A joint decision with the patient requires a comprehensive assessment of prognosis and multidisciplinary counseling. If screening or other ultrasound findings are suggestive of a common aneuploidy, initially a karyotype analysis and fluorescence in situ hybridization should be performed. If these test results are normal, a chromosomal microarray should be recommended to the family [10].
Conclusion
This report demonstrates the importance of a systematic evaluation of all fetal organs, especially the cardiovascular system, urogenital system, and hematopoietic system when a radial ray defect is detected on ultrasonography. Although the number of cases in our study was limited, it was important for raising awareness in cases with radial ray defects to identify factors such as VACTERL association, trisomy 18, Fanconi anemia, and amniotic band syndrome that may be involved in the etiology.
The limitations of our study include the fact that it was a retrospective study, that the cases were evaluated at late gestational weeks due to being a reference center, that the rate of acceptance of the karyotype analysis was low, that the patients rejected further genetic and autopsy examinations after termination, and that there was a lack of additional syndromic diagnosis.
This study demonstrates that advanced genetic and sonographic evaluation of the fetus in cases with radial ray defects is necessary for clinical management and appropriate family counseling.
Zdroje
1. Pakkasjärvi N, Koskimies E, Ritvanen A et al. Characteristics and associated anomalies in radial ray deficiencies in Finland – a population‐based study. Am J Med Genet A 2013; 161 (2): 261–267. doi: 10.1002/ajmg.a.35707.
2. Koskimies E, Lindfors N, Gissler M et al. Congenital upper limb deficiencies and associated malformations in Finland: a population-based study. J Hand Surg Am 2011; 36 (6): 1058–1065. doi: 10.1016/j.jhsa.2011.03.015.
3. Goldfarb CA, Wall L, Manske PR. Radial longitudinal deficiency: the incidence of associated medical and musculoskeletal conditions. J Hand Surg Am 2006; 31 (7): 1176–1182. doi: 10.1016/ j.jhsa.2006.05.012.
4. Giele H, Giele C, Bower C et al. The incidence and epidemiology of congenital upper limb anomalies: a total population study. J Hand Surg Am 2001; 26 (4): 628–634. doi: 10.1053/jhsu. 2001.26121.
5. Barham G, Clarke NM. Genetic regulation of embryological limb development with relation to congenital limb deformity in humans. J Child Orthop 2008; 2 (1): 1–9. doi: 10.1007/s11832-008-0076-2.
6. Black AJ, Lu DY, Yefet LS et al. Sex differences in surgically correctable congenital anomalies: a systematic review. J Pediatr Surg 2020; 55 (5): 811–820. doi: 10.1016/j.jpedsurg.2020.01.016.
7. Al-Qattan MM. The classification of VACTERL association into 3 groups according to the limb defect. Plast Reconstr Surg Glob Open 2021; 9 (2): e3360. doi: 10.1097/gox.0000000000003360.
8. Rittler M, Paz JE, Castilla EE. VACTERL association, epidemiologic definition and delineation. Am J Med Genet 1996; 63 (4): 529–536. doi: 10.1002/ (SICI) 1096-8628 (19960628) 63 : 4<529:: AID-AJMG4>3.0.CO; 2-J.
9. Alter BP, Rosenberg PS. VACTERL-H association and Fanconi anemia. Mol Syndromol 2013; 4 (1–2): 87–93. doi: 10.1159/0003-46035.
10. Avcı Ş, Toksoy G, Bağırova G et al. Clinical classification of radial ray defects and research into etiopathogenesis. J Ist Faculty Med 2018; 81 (4): 127–138. doi: 10.26650/IUITFD.427250.
ORCID of authors
G. Ünver 0000-0002-0887-2634
S. Serin 0000-0003-2477-138X
M. Tosun 0000-0003-1548-5111
H. Çelik 0000-0001-5201-9385
M. Önal 0000-0003-1222-3386
Ü. Abur 0000-0002-4811-9321
E. Altundağ 0000-0001-8841-1426
Authorship
GU, SS and MT collaborated on designing the study, collecting and analyzing the data, and writing the manuscript.
GU, HC and MO contributed to designing the study, collecting data, and editing the manuscript. UA and EA assisted with data analysis and interpretation.
GU, MT, UA and MO provided critical feedback and made revisions to the manuscript.
All authors reviewed and approved the final version of the manuscript for submission.
Submitted/Doručeno: 26. 9. 2025
Accepted/Přijato: 5. 10. 2025
Gökhan Ünver, MD
Department of Obstetrics and Gynecology
Perinatology Unit
Faculty of Medicine
Ondokuz Mayis University
55200 Atakum/Samsun
Turkey
drgokhanunver@outlook.com
Štítky
Dětská gynekologie Gynekologie a porodnictví Reprodukční medicínaČlánek vyšel v časopise
Česká gynekologie

2026 Číslo 1
Nejčtenější v tomto čísle
- Pelvic floor muscles High-Intensity Tesla Stimulation
- Cervical cancer screening in the European context – from cytology to primary HPV testing
- Molar ectopic pregnancy in a cesarean scar treated with methotrexate – a case report and review of the literature
- Cytological versus histological results in ASCUS cervical dysplasia – a retrospective study