
Robotic interposition of the mesorectum during low anterior resection of the rectum for endometriosis using tissue perfusion assessment with indocyanine green
Authors:
Vladimír Baláž 1,2
![]() ; V. Teplan 3; K. Benková 4; Jiří Presl 5
; V. Teplan 3; K. Benková 4; Jiří Presl 5
![]()
Authors place of work:
Department of Gynecology, Motol and Homolka University Hospital, Prague
1; Faculty of Medicine, Charles University, Pilsen
2; Department of Surgery, Motol and Homolka University Hospital, Prague
3; Department of Pathology, Motol and Homolka University Hospital, Prague
4; Department of Gynecology and Obstetrics, University Hospital, Pilsen
5
Published in the journal:
Ceska Gynekol 2026; 91(1): 46-51
Category:
Kazuistika
doi:
https://doi.org/10.48095/cccg202646
Summary
Introduction: Rectal endometriosis is a serious disease, and its surgical treatment belongs among demanding procedures, often requiring a multidisciplinary approach. It is associated with a significant risk of peri - and postoperative complications, the most serious being the development of rectovaginal fistula, which may occur in up to 10% of resections for rectal endometriosis. Preventive measures include the choice of surgical technique, such as a two-stage procedure (resection with terminal stoma followed by stoma closure and bowel anastomosis), which is not optimal for the patient due to the necessity of having two surgeries. Another option is the interposition of the patient’s vital tissues into the site of anastomosis or intestinal wall suture. For this purpose, an omental flap is often used, or part of the mesorectum may be utilized. The ability to verify the vitality of such a flap should be considered crucial in preventing anastomotic leakage. Methods: A patient underwent robotic-assisted laparoscopic segmental resection of severe rectal endometriosis involving the rectovaginal septum and vagina, classified as #ENZIAN A3 and C3, with interposition of the mesorectum and intraoperative tissue perfusion assessment using indocyanine green. Conclusion: The use of tissue perfusion assessment when performing interposition of patient-derived flaps may, in the future, improve surgical precision, enhance success rates, and contribute to the prevention of rectovaginal fistula formation.
Keywords:
indocyanine green – tissue perfusion – deep rectal endometriosis – segmental resection – rectovaginal fistula – mesorectum
Introduction
Endometriosis affects 7–10% of women of reproductive age [1]. The most severe manifestation is deep infiltrating endometriosis, occurring in 5–12% of patients with the disease [2]. It most commonly involves the posterior compartment, including the cervix and vaginal fornix, with secondary infiltration of the anterior rectal wall [1]. Pharmacological treatment may suppress symptoms but does not cure the disease. Surgical excision is often the only option to relieve symptoms affecting urinary, intestinal, sexual, and reproductive function [1].
The gold standard consists of three surgical techniques: rectal shaving (nodule excision), discoid resection, and segmental resection. No consensus exists on the optimal procedure, and selection remains debated, with significant room for individualized approaches depending on findings and patient symptoms. Given complication risks and recurrence of pain, nodule excision is the least burdensome procedure, while segmental resection is the most demanding. However, this may be explained by the fact that segmental resections are often reserved for the most severe cases [1].
Surgery can be performed via open, laparoscopic, or robot-assisted approaches. Although no significant differences in patient outcomes were found when comparing laparoscopy and robot-assisted laparoscopy [3], the robotic approach offers surgeons better visualization and increased ergonomic comfort.
The most frequent complications of segmental resection, regardless of approach, are rectovaginal fistula and anastomotic leakage [1], with reported risk rates up to 10% [1]. Risk factors include the level of rectal involvement, with higher risk with the lesion near the anorectal junction accompanied with the intraoperative vaginal opening [1], excessive use of electrocoagulation in the posterior fornix with associated ischemia [4], and the lesion size greater than 4 cm [4], although the latter remains debated [2].
Preventive measures include interposition of patient tissue between resection margins, with or without protective stoma, or performing the surgery in two stages [5]. Omental flap has been used with some success but this is technically challenging due to anatomical position of omentum [6]. Therefore mesorectal flap has been used as substitute [6]. Since endometriosis is a benign disease, total mesorectal excision (TME) is not necessary, and the mesorectum can be preserved in situ. Intraoperative evaluation of tissue vitality can be facilitated by indocyanine green (ICG), a fluorescent dye used for perfusion assessment [7]. After intravenous application, it emits near-infrared radiation when excited. It has good bioavailability, a short half-life, and a unique safety profile, and has been used in medicine for nearly 70 years [7].
Material and method
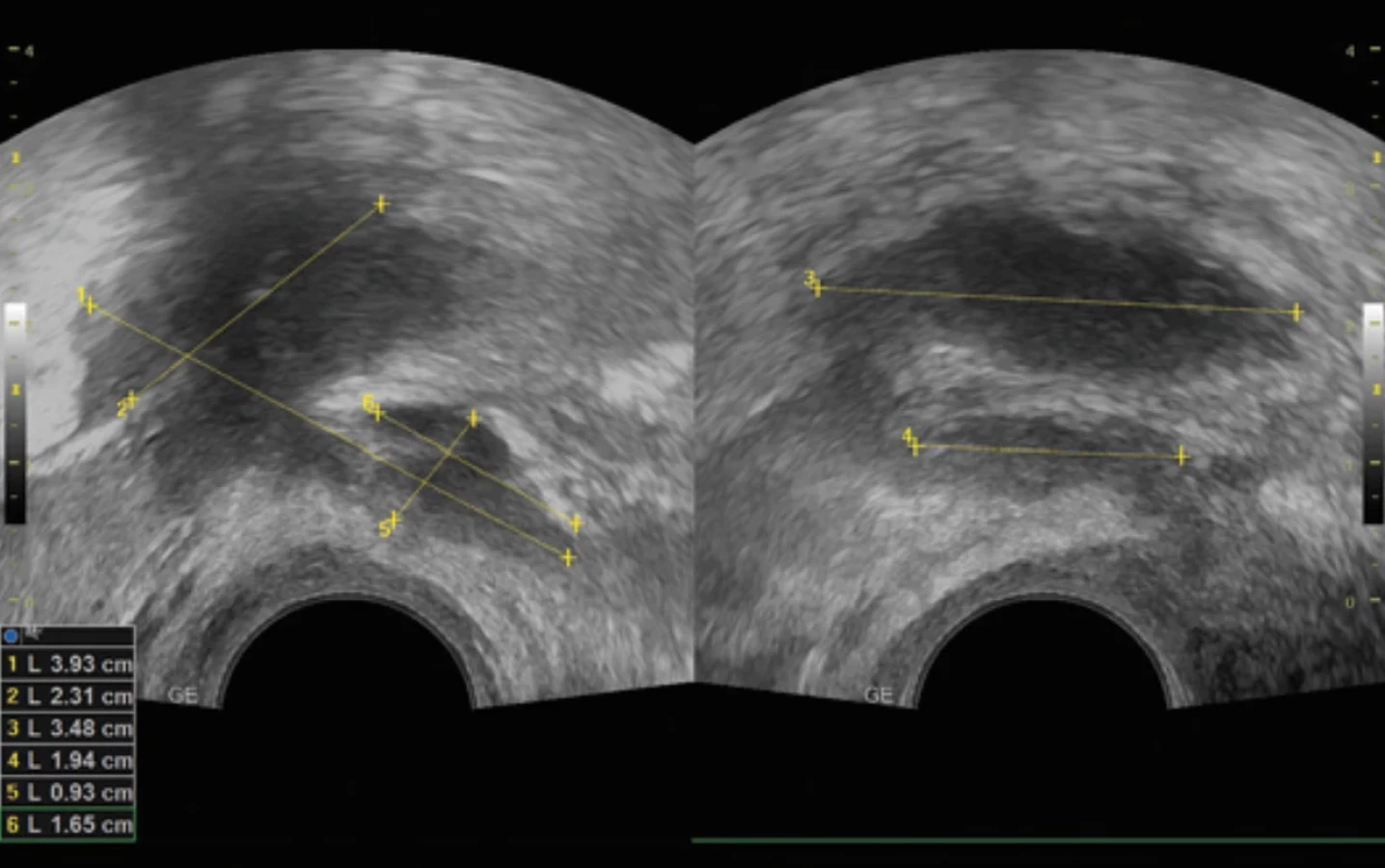
A 39-year-old nulligravida, nullipara in care of a center for assisted reproduction. Her history included three laparoscopic surgeries for endometriosis including the major resection of deep infiltrating endometriosis of the vaginal fornix in 2023. She attempted pregnancy approximately one and a half years since her last surgery. She was referred to our department from the fertility center after two natural cycles. Preoperative tests showed low AMH levels. A recurrent endometriotic nodule was found in the posterior fornix, rectum, and sigmoid colon (#ENZIAN (u) A3, C3, T2/x, FI) (Fig. 1), confirmed by MRI. Clinically, she reported minimal to no symptoms. Due to the findings and planned IVF and after discussion with the patient we agreed on a robotic-assisted laparoscopic segmental resection of the rectum and vaginal fornix.
The procedure was performed under general anesthesia using the Da Vinci Xi system, with the participation of the colorectal surgeon.
Intraoperative finding was classified as #ENZIAN (s) A3, C3, T3/2, FI (Fig. 2). Extensive adhesiolysis (grade IV) was necessary. After mobilization of the rectosigmoid, resection of the posterior vaginal fornix was performed (provided with suture), followed by low anterior resection of the rectum with end-to-end anastomosis using a 31 mm circular stapler. The level of resection was confirmed using perfusion assessment of the intestinal wall with bolus intravenous application of 25 mg of indocyanine green [7]. The rectal specimen was removed and stapler head constructed through a mini-laparotomy in the left lower abdomen. After construction of the end-to-end anastomosis, a mesorectal flap was prepared and after confirming its perfusion with indocyanine green (the same observation window as mentioned above) (Fig. 3), was interposed and fixed with absorbable sutures do interstinal wall, between the vaginal suture and the intestinal anastomosis (Fig. 4). A rectal tube was placed across the anastomosis for 48 hours.



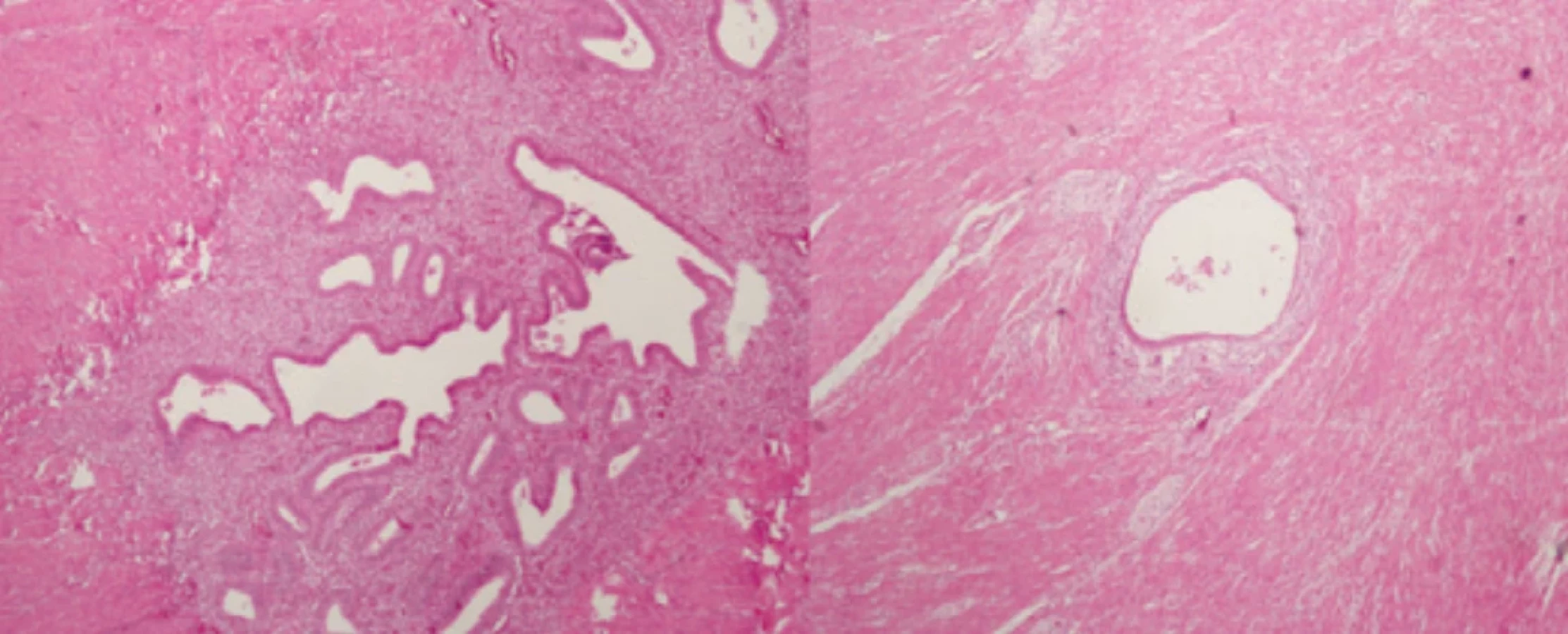
The rectosigmoid specimen contained two nodules: one in the rectum measuring 5 × 3 cm (consistent with ultrasound findings) and another about 12 cm proximal, measuring 4 × 3 cm, which narrowed the sigmoid lumen to 2 cm (Fig. 5, 6).

Postoperative recovery was uneventful, with passage of gases and stool on days 2 and 4, resp. The patient was discharged on 7th postoperative day. Follow-up every 14 days up to 6 weeks showed no complications. The presence of the mesorectal flap was confirmed postoperatively by ultrasound via the posterior fornix.
Five months after the surgery, the patient conceived through assisted reproduction with a donated oocyte, but the pregnancy ended as an anembryonic gestation, with the necessity for instrumental revision.

Discussion
Decision-making regarding which surgical procedure to perform in such patients is extremely challenging, with no clear consensus. An individualized approach is preferred. Some authors have attempted to propose algorithms based on clinical experience and expertise, considering symptomatology, lesion size, and number of lesions. Shaving is recommended for unifocal nodules up to 2–3 cm, discoid resection for incomplete shaving, and segmental resection for multifocal lesions [1]. Another factor is the depth of invasion, which is difficult to assess preoperatively. Lesions affecting 40% or more of the bowel circumference have an 89.3% probability of involvement of the submucosal and mucosal layers, though this has only been confirmed in resection specimens, not preoperatively by ultrasound or magnetic resonance imaging [8].
Another factor to consider is the risk of residual disease. Due to complication risks, less invasive procedures (shaving) may be preferable [1]. However, after nodule excision, residual disease may remain in more than 19.2% of cases [9], and in 14.6% of colorectal resections, residual disease may even be present at the resection margin [10]. Although this does not seem to have effect in short-term outcomes [10]. In most of the cases, especially in larger nodules, the nodule margin contains fibrosis and metaplastic smooth muscle with a hypoperfusion pattern, which may be assessed by using fluorescent dye during nodule excision [7].
Conclusion
Ischemia plays a key role in the pathogenesis of rectovaginal fistulas. Preventing ischemia through minimally destructive resection techniques and real-time perfusion assessment with indocyanine green may help to prevent rectovaginal fistulas and other complications associated with postoperative ischemia in the affected area.
Zdroje
1. Donnez O, Roman H. Choosing the right surgical technique for deep endometriosis: shaving, disc excision, or bowel resection? Fertil Steril 2017; 108 (6): 931–942. doi: 10.1016/j.fertnstert.2017.09.006.
2. Zheng Y, Zhang N, Lu W et al. Rectovaginal fistula following surgery for deep infiltrating endometriosis: does lesion size matter? J Int Med Res 2018; 46 (2): 852–864. doi: 10.1177/0300 060517728208.
3. Pavone M, Baroni A, Campolo F et al. Robotic assisted versus laparoscopic surgery for deep endometriosis: a meta-analysis of current evidence. J Robot Surg 2024; 18 (1): 212. doi: 10.1007/s11701-024-01954-2.
4. Meuleman C, Tomassetti C, D’Hoore A et al. Surgical treatment of deeply infiltrating endometriosis with colorectal involvement. Hum Reprod Update 2011; 17 (3): 311–326. doi: 10.1093/humupd/dmq057.
5. Kondo W, Bourdel N, Tamburro S et al. Complications after surgery for deeply infiltrating pelvic endometriosis. BJOG 2011; 118 (3): 292–298. doi: 10.1111/j.1471-0528.2010.02774.x.
6. Hanacek J, Havluj L, Drahonovsky J et al. Interposition of the mesorectal flap as prevention of rectovaginal fistula in patients with endometriosis. Int Urogynecol J 2019; 30 (12): 2195–2198. doi: 10.1007/s00192-019-04030-8.
7. Baláž V, Syrůček M, Presl J. Possible use of indocyanine green in the management of endometriosis. Ceska Gynekol 2025; 90 (3): 238–246. doi: 10.48095/cccg2025238.
8. Abrão MS, Podgaec S, Dias JA Jr et al. Endometriosis lesions that compromise the rectum deeper than the inner muscularis layer have more than 40% of the circumference of the rectum affected by the disease. J Minim Invasive Gynecol 2008; 15 (3): 280–285. doi: 10.1016/ j.jmig.2008.01.006.
9. Remorgida V, Ragni N, Ferrero S et al. How complete is full thickness disc resection of bowel endometriotic lesions? A prospective surgical and histological study. Hum Reprod 2005; 20 (8): 2317–2320. doi: 10.1093/humrep/dei047.
10. Roman H, Hennetier C, Darwish B et al. Bowel occult microscopic endometriosis in resection margins in deep colorectal endometriosis specimens has no impact on short-term postoperative outcomes. Fertil Steril 2016; 105 (2): 423.e7–429.e7. doi: 10.1016/j.fertnstert.2015.09.030.
ORCID of authors
V. Baláž 0009-0007-7387-2191
J. Presl 0000-0001-7632-4069
Submitted/Doručeno: 5. 10. 2025
Accepted/Přijato: 8. 10. 2025
Vladimír Baláž, MD
Department of Gynecology
Motol and Homolka University Hospital
Roentgenova 37/2
150 00 Praha 5
Prague
vladimir.balaz@fnmh.cz
Štítky
Dětská gynekologie Gynekologie a porodnictví Reprodukční medicínaČlánek vyšel v časopise
Česká gynekologie

2026 Číslo 1
Nejčtenější v tomto čísle
- Pelvic floor muscles High-Intensity Tesla Stimulation
- Cervical cancer screening in the European context – from cytology to primary HPV testing
- Molar ectopic pregnancy in a cesarean scar treated with methotrexate – a case report and review of the literature
- Cytological versus histological results in ASCUS cervical dysplasia – a retrospective study